

Challenges in pulmonary hypertension: managing the unexpected
- PMID: 26621981
- PMCID: PMC9487621
- DOI: 10.1183/16000617.0060-2015
Challenges in pulmonary hypertension: managing the unexpected
Abstract
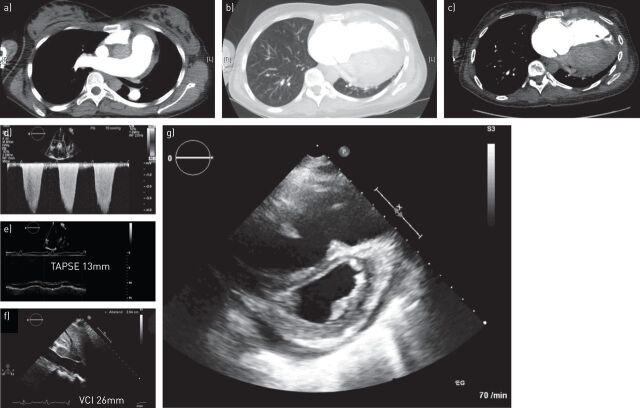
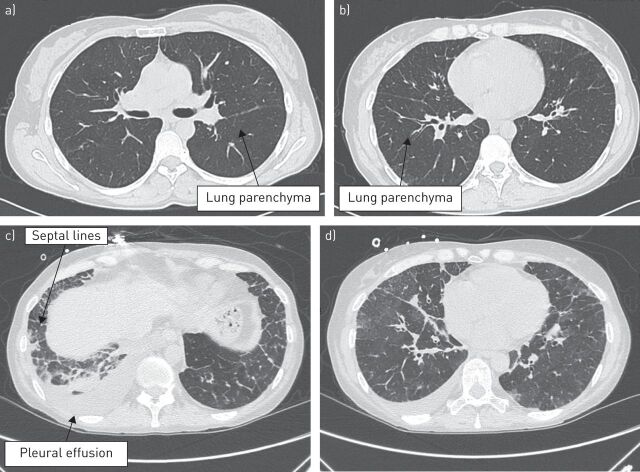
The diverse challenges associated with diagnosis and management of patients with pulmonary hypertension are illustrated in this case-based review. Case 1 describes a patient diagnosed with pulmonary arterial hypertension (PAH) with right heart failure and active systemic lupus erythematosus who was effectively treated with an up-front triple combination of PAH therapies and immunosuppressive therapy. In case 2, a diagnosis of pulmonary veno-occlusive disease was reached after a combined approach of clinical suspicion, physical examination, and invasive and noninvasive tests. Cautious PAH therapy and high-dose diuretics provided clinical benefit in this patient and served as a bridge to lung transplantation. These cases highlight the need for ongoing follow-up of patients with PAH, comprising frequent assessment of treatment success and continued diagnostic evaluation.
Copyright ©ERS 2015.
Conflict of interest statement
Conflict of interest: Disclosures can be found alongside the online version of this article at
Figures
References
-
- Galiè N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J 2015. [In press DOI: 10.1093/eurheartj/ehv317].
-
- Galiè N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J 2015; 46: 903–975. - PubMed
-
- Winslow TM, Ossipov MA, Fazio GP, et al. Five-year follow-up study of the prevalence and progression of pulmonary hypertension in systemic lupus erythematosus. Am Heart J 1995; 129: 510–515. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical