

General practice funding underpins the persistence of the inverse care law: cross-sectional study in Scotland
- PMID: 26622032
- PMCID: PMC4655733
- DOI: 10.3399/bjgp15X687829
General practice funding underpins the persistence of the inverse care law: cross-sectional study in Scotland
Abstract
Background: Universal access to health care, as provided in the NHS, does not ensure that patients' needs are met.
Aim: To explore the relationships between multimorbidity, general practice funding, and workload by deprivation in a national healthcare system.
Design and setting: Cross-sectional study using routine data from 956 general practices in Scotland.
Method: Estimated numbers of patients with multimorbidity, estimated numbers of consultations per 1000 patients, and payments to practices per patient are presented and analysed by deprivation decile at practice level.
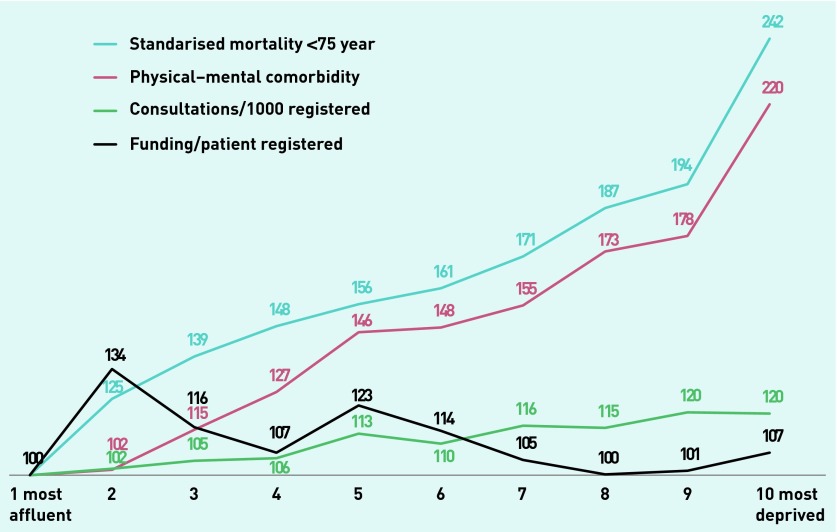
Results: Levels of multimorbidity rose with practice deprivation. Practices in the most deprived decile had 38% more patients with multimorbidity compared with the least deprived (222.8 per 1000 patients versus 161.1; P<0.001) and over 120% more patients with combined mental-physical multimorbidity (113.0 per 1000 patients versus 51.5; P<0.001). Practices in the most deprived decile had 20% more consultations per annum compared with the least deprived (4616 versus 3846, P<0.001). There was no association between total practice funding and deprivation (Spearman ρ -0.09; P = 0.03). Although consultation rates increased with deprivation, the social gradients in multimorbidity were much steeper. There was no association between consultation rates and levels of funding.
Conclusion: No evidence was found that general practice funding matches clinical need, as estimated by different definitions of multimorbidity. Consultation rates provide only a partial estimate of the work involved in addressing clinical needs and are poorly related to the prevalence of multimorbidity. In these circumstances, general practice is unlikely to mitigate health inequalities and may increase them.
Keywords: consultation rates; funding; general practice; inverse care law; multimorbidity.
© British Journal of General Practice 2015.
Figures
Comment in
-
Multimorbidity and GP burnout.Br J Gen Pract. 2020 Feb 27;70(692):108. doi: 10.3399/bjgp20X708353. Print 2020 Mar. Br J Gen Pract. 2020. PMID: 32107218 Free PMC article. No abstract available.
Similar articles
-
Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study.Lancet. 2012 Jul 7;380(9836):37-43. doi: 10.1016/S0140-6736(12)60240-2. Epub 2012 May 10. Lancet. 2012. PMID: 22579043
-
The influence of socioeconomic deprivation on multimorbidity at different ages: a cross-sectional study.Br J Gen Pract. 2014 Jul;64(624):e440-7. doi: 10.3399/bjgp14X680545. Br J Gen Pract. 2014. PMID: 24982497 Free PMC article.
-
Multimorbidity and Socioeconomic Deprivation in Primary Care Consultations.Ann Fam Med. 2018 Mar;16(2):127-131. doi: 10.1370/afm.2202. Ann Fam Med. 2018. PMID: 29531103 Free PMC article.
-
Current experience and future potential of facilitating access to digital NHS primary care services in England: the Di-Facto mixed-methods study.Health Soc Care Deliv Res. 2024 Sep;12(32):1-197. doi: 10.3310/JKYT5803. Health Soc Care Deliv Res. 2024. PMID: 39324475 Review.
-
Impact of telephone triage on access to primary care for people living with multiple long-term health conditions: rapid evaluation.Southampton (UK): National Institute for Health and Care Research; 2022 Jun. Southampton (UK): National Institute for Health and Care Research; 2022 Jun. PMID: 35793423 Free Books & Documents. Review.
Cited by
-
Resources in vulnerable young adults: self-assessments during preventive consultation with their general practitioner in Denmark.Health Promot Int. 2020 Oct 1;35(5):1180-1189. doi: 10.1093/heapro/daz114. Health Promot Int. 2020. PMID: 31750922 Free PMC article. Clinical Trial.
-
Professional resilience in GPs working in areas of socioeconomic deprivation: a qualitative study in primary care.Br J Gen Pract. 2018 Dec;68(677):e819-e825. doi: 10.3399/bjgp18X699401. Epub 2018 Oct 8. Br J Gen Pract. 2018. PMID: 30297436 Free PMC article.
-
Multimorbidity and GP burnout.Br J Gen Pract. 2020 Feb 27;70(692):108. doi: 10.3399/bjgp20X708353. Print 2020 Mar. Br J Gen Pract. 2020. PMID: 32107218 Free PMC article. No abstract available.
-
Mining for Deep End GPs: a group forged with steel in Yorkshire and Humber.Br J Gen Pract. 2017 Jan;67(654):36-37. doi: 10.3399/bjgp17X688765. Br J Gen Pract. 2017. PMID: 28034948 Free PMC article. No abstract available.
-
Green social prescribing: challenges and opportunities to implementation in deprived areas.Br J Gen Pract. 2023 Jul 27;73(733):342-343. doi: 10.3399/bjgp23X734409. Print 2023 Aug. Br J Gen Pract. 2023. PMID: 37500466 Free PMC article. No abstract available.
References
-
- Starfield B. Contributions of evidence to the struggle towards equity. Nuffield Trust: Nuffield Trust For Research and Policy Studies in Health Services; 2004. John Fry Fellowship Lecture.
-
- Hart JT. The inverse care law. Lancet. 1971;297:405–412. - PubMed
-
- Watt G. The inverse care law today. Lancet. 2002;360:252–254. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous