

Alternatively activated macrophages are associated with metastasis and poor prognosis in prostate adenocarcinoma
- PMID: 26622679
- PMCID: PMC4533309
- DOI: 10.3892/ol.2015.3400
Alternatively activated macrophages are associated with metastasis and poor prognosis in prostate adenocarcinoma
Abstract
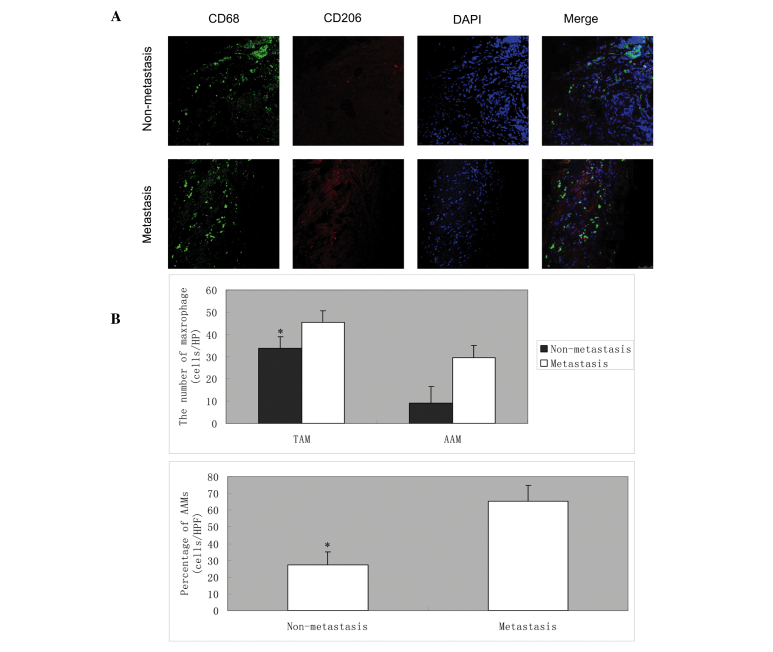
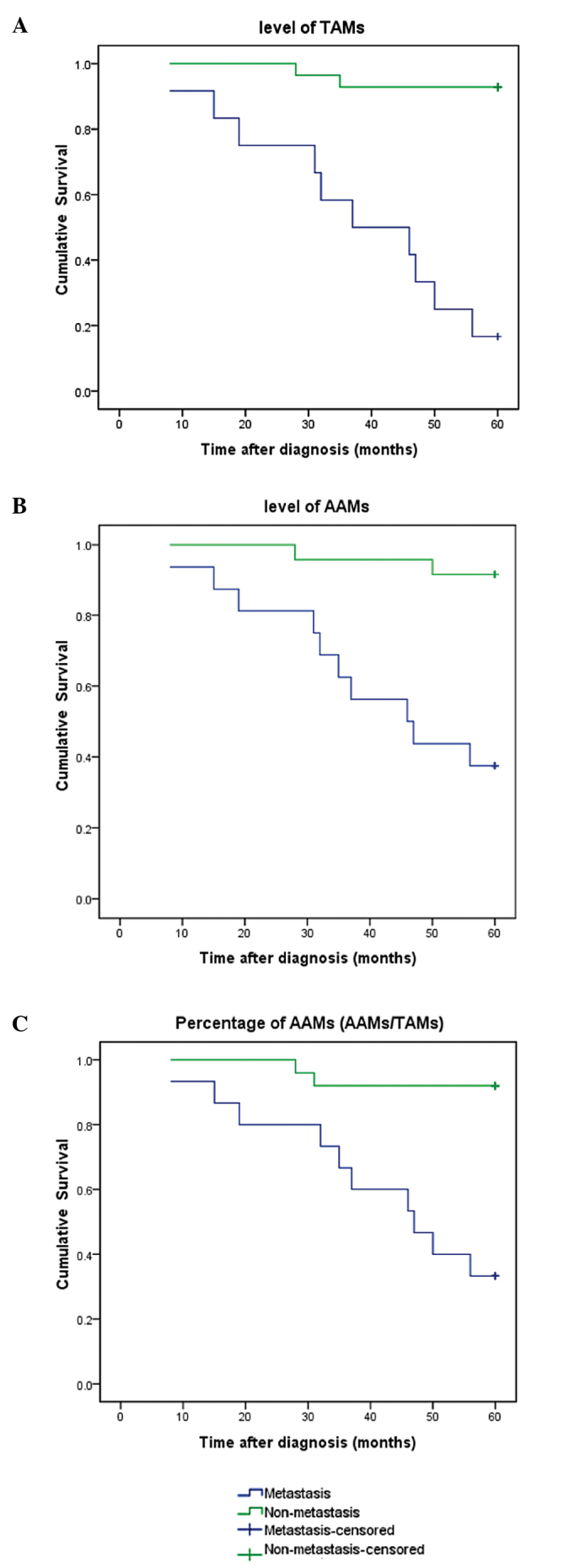
Recent studies have revealed that alternatively activated macrophages (AAMs) are involved in tumor progression. However, the effect of AAMs on the metastasis of prostate cancer is poorly understood. In the present study, the prostate tissues of 42 patients with prostate adenocarcinoma (PCa) were used in the analysis of tumor associated macrophages (TAMs) and AAMs by immunofluorescence. The patients were followed up for 5 years. The associations of TAMs and AAMs with the clinicopathological features and outcome in these cases were evaluated. Immunofluorescent analysis indicated that the mean number of TAMs (CD68-positive cells) in the prostate tissues of PCa patients with metastasis [45.29±7.25 cells/high-power field (HPF)] was significantly higher compared with that of PCa patients without metastasis (33.57±5.25 cells/HPF; P<0.01). The mean numbers of AAMs (CD68- and CD206-positive cells) in the tissues of PCa patients with and without metastasis were 29.43±5.68 and 9.14±5.29 cells/HPF, respectively. In addition, the percentage of AAMs (number of AAMs/number of TAMs) was 65.11±9.68 and 27.32±7.85% in patients with and without metastasis, respectively. The differences in the number and percentage of AAMs between the two groups were statistically significant (P<0.01). The number and percentage of AAMs was positively correlated with tumor grade and serum prostate-specific antigen (PSA) level. Univariate analysis indicated that the level of PSA, Gleason score, metastatic status, T grade, number of TAMs, number of AAMs and percentage of AAMs were predictors of the overall survival. Furthermore, multivariate analyses revealed that Gleason score, level of PSA and number of TAMs were predictors for overall survival rate. These results indicate that TAMs and AAMs may be important in the metastasis of PCa, and that TAMs and AAMs may be used as potential biomarkers of poor prognosis in late-stage PCa patients.
Keywords: alternatively activated macrophage; metastasis; prognosis; prostate adenocarcinoma; tumor associated macrophage.
Figures
References
-
- Han SJ, Zhang SW, Chen WQ, Li CL. Analysis of status and trends of prostate cancer incidence in China. Lin chuang Zhong Liu Xue Za Zhi. 2013;18:330–335.
-
- Loblaw DA, Virgo KS, Nam R, et al. American Society of Clinical Oncology : Initial hormonal management of androgen-sensitive metastatic, recurrent, or progressive prostate cancer: 2006 update of an American Society of Clinical Oncology practice guideline. J Clin Oncol. 2007;25:1596–1605. doi: 10.1200/JCO.2006.10.1949. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous