

Digital versus traditional air leak evaluation after elective pulmonary resection: a prospective and comparative mono-institutional study
- PMID: 26623093
- PMCID: PMC4635273
- DOI: 10.3978/j.issn.2072-1439.2015.09.12
Digital versus traditional air leak evaluation after elective pulmonary resection: a prospective and comparative mono-institutional study
Abstract
Background: The increased demand to reduce costs and hospitalization in general pushed several institution worldwide to develop fast-tracking protocols after pulmonary resections. One of the commonest causes of protracted hospital stay remains prolonged air leaks (ALs). We reviewed our clinical practice with the aim to compare traditional vs. digital chest drainages in order to evaluate which is the more effective to correctly manage the chest tube after pulmonary resection.
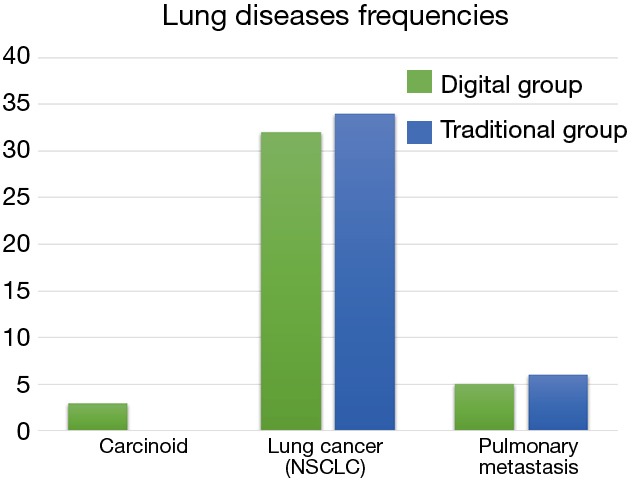
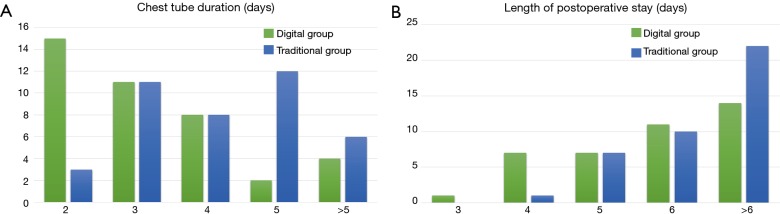
Methods: All patients submitted to elective pulmonary resection for lung malignancies, between April to December, 2014 in our General Thoracic Surgery Department were included in the study. The primary outcome was the chest tube duration, the secondary the postoperative overall hospitalization. Significant differences between traditional and digital groups were investigated with logistic regression models. Numerical variables between the groups were compared by means of the unpaired Wilcoxon-Mann-Whitney test.
Results: Both series of patients were comparable for clinical, surgical and pathological characteristics. Chest tube duration showed to be significantly shorter in the digital group (3 vs. 5 days, P=0.0009), while the hospitalization was longer in traditional one [8 vs. 7 days in digital drainage (DD); P=0.0385]. No chest drainage replacement was required at 30-day, in both groups.
Conclusions: We were able to demonstrate that patients managed with a digital system experienced a shorter chest tube duration as well as a lower overall hospital length of stay, compared to those who received the traditional drainage (TD).
Keywords: Air leak (AL); chest drainage; digital chest drainage system; postoperative management; traditional chest drainage system.
Conflict of interest statement
Figures

References
-
- Cerfolio RJ, Pickens A, Bass C, et al. Fast-tracking pulmonary resections. J Thorac Cardiovasc Surg 2001;122:318-24. - PubMed
-
- Cerfolio RJ, Bass CS, Pask AH, et al. Predictors and treatment of persistent air leaks. Ann Thorac Surg 2002;73:1727-30; discussion 1730-1. - PubMed
-
- Antanavicius G, Lamb J, Papasavas P, et al. Initial chest tube management after pulmonary resection. Am Surg 2005;71:416-9. - PubMed
-
- Brunelli A, Monteverde M, Borri A, et al. Predictors of prolonged air leak after pulmonary lobectomy. Ann Thorac Surg 2004;77:1205-10; discussion 1210. - PubMed
-
- Varela G, Jiménez MF, Novoa NM, et al. Postoperative chest tube management: measuring air leak using an electronic device decreases variability in the clinical practice. Eur J Cardiothorac Surg 2009;35:28-31. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous