

Clinical feasibility and efficacy of video-assisted thoracic surgery (VATS) anatomical resection in patients with central lung cancer: a comparison with thoracotomy
- PMID: 26623100
- PMCID: PMC4635295
- DOI: 10.3978/j.issn.2072-1439.2015.10.32
Clinical feasibility and efficacy of video-assisted thoracic surgery (VATS) anatomical resection in patients with central lung cancer: a comparison with thoracotomy
Abstract
Background: The aim of this study is to evaluate the clinical feasibility and efficacy of video-assisted thoracoscopic surgery (VATS) anatomical pulmonary resection in patients with central lung cancer.
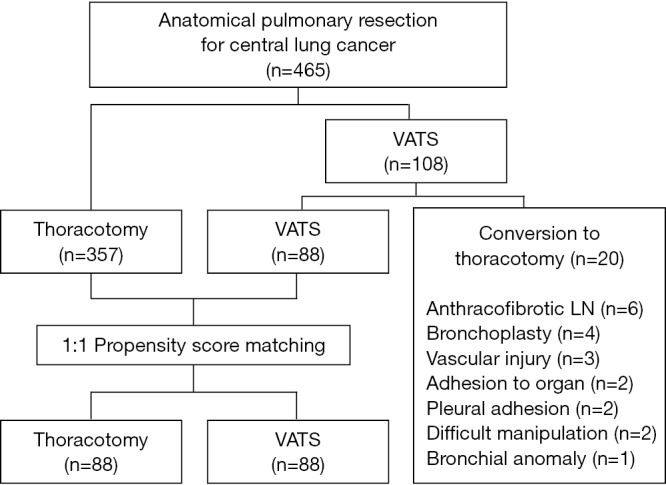
Methods: Between July 2004 and December 2011, 465 patients underwent anatomical pulmonary resection and systematic mediastinal lymph node sampling or dissection for central lung cancer. Because patients were not randomized to receive VATS, clinical outcomes were compared using a propensity score matching design, giving 88 patients in each group.
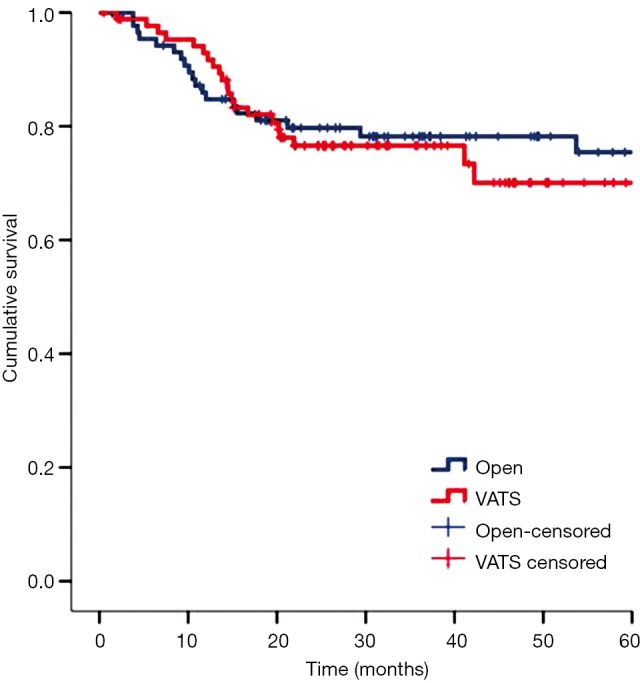
Results: A lobectomy was attempted in 69 patients of the thoracotomy group and 64 of the VATS group, bilobectomy in 19 patients of the thoracotomy group and 21 of the VATS group, and segmentectomy in 3 patients of the VATS group. There were no differences in the anatomical distribution of pulmonary resections between the two groups. There was no operation related in-hospital mortality. There were 34 postoperative complications in 30 patients, without significant differences between the two groups. The median hospital stay and chest tube indwelling period of the VATS group were shorter than those of the thoracotomy group by 2 days and 1 day, respectively (P<0.05). During a median follow-up of 32.5 months (range, 0.5-95.8 months), there was no difference between the two groups in 3-year recurrence-free or overall survivals (OS).
Conclusions: VATS anatomical pulmonary resection is safe and feasible for central lung cancer, providing a low operative mortality and favorable outcomes in selected patients. Further case studies with long-term outcome data are necessary to verify our conclusions.
Keywords: Central lung cancer; anatomical pulmonary resection; thoracotomy; video-assisted thoracoscopic surgery (VATS).
Conflict of interest statement
Figures

References
-
- Lewis RJ, Sisler GE, Caccavale RJ. Imaged thoracic lobectomy: should it be done? Ann Thorac Surg 1992;54:80-3. - PubMed
-
- Daniels LJ, Balderson SS, Onaitis MW, et al. Thoracoscopic lobectomy: a safe and effective strategy for patients with stage I lung cancer. Ann Thorac Surg 2002;74:860-4. - PubMed
-
- Swanson SJ, Meyers BF, Gunnarsson CL, et al. Video-assisted thoracoscopic lobectomy is less costly and morbid than open lobectomy: a retrospective multiinstitutional database analysis. Ann Thorac Surg 2012;93:1027-32. - PubMed
-
- Yim AP. VATS major pulmonary resection revisited--controversies, techniques, and results. Ann Thorac Surg 2002;74:615-23. - PubMed
-
- Takamochi K, Yokose T, Yoshida J, et al. Calcification in large cell neuroendocrine carcinoma of the lung. Jpn J Clin Oncol 2003;33:10-3. - PubMed
LinkOut - more resources
Full Text Sources