

Automatic Craniomaxillofacial Landmark Digitization via Segmentation-Guided Partially-Joint Regression Forest Model and Multiscale Statistical Features
- PMID: 26625402
- PMCID: PMC4879598
- DOI: 10.1109/TBME.2015.2503421
Automatic Craniomaxillofacial Landmark Digitization via Segmentation-Guided Partially-Joint Regression Forest Model and Multiscale Statistical Features
Abstract
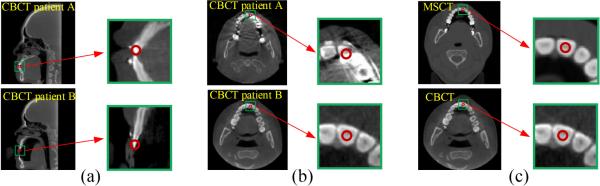
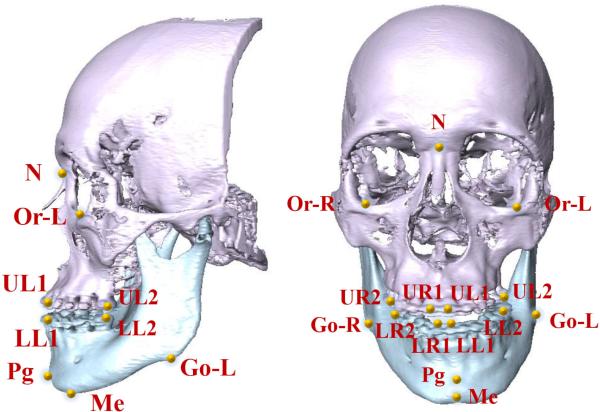
Objective: The goal of this paper is to automatically digitize craniomaxillofacial (CMF) landmarks efficiently and accurately from cone-beam computed tomography (CBCT) images, by addressing the challenge caused by large morphological variations across patients and image artifacts of CBCT images.
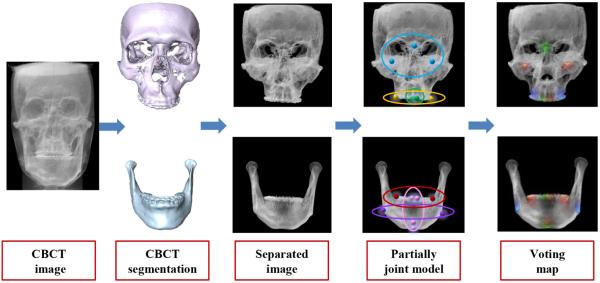
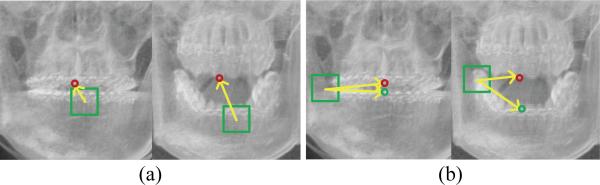
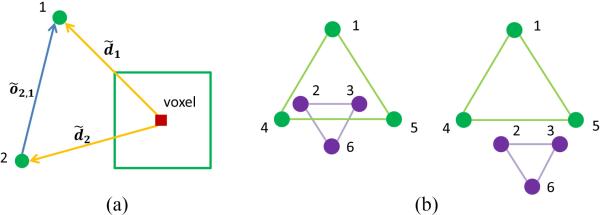
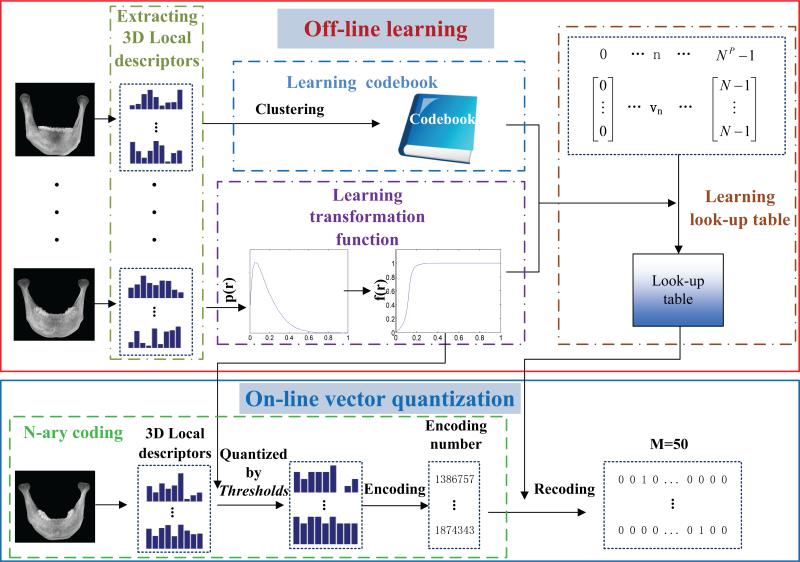
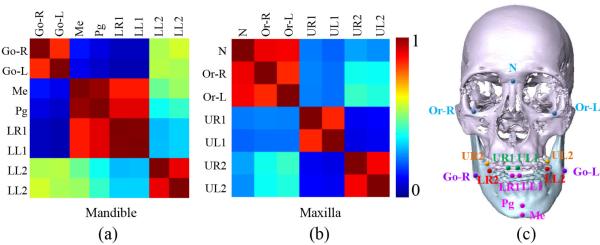
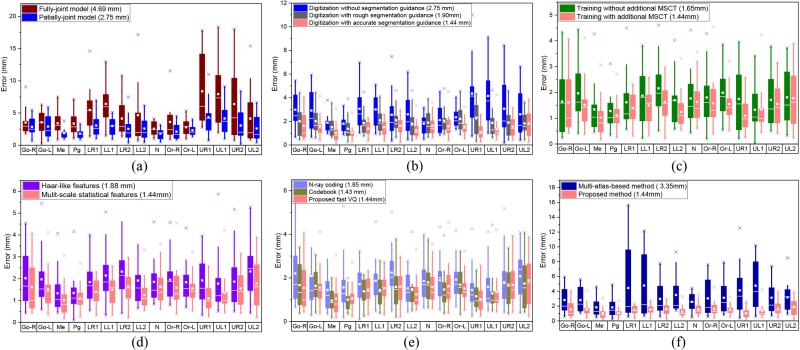
Methods: We propose a segmentation-guided partially-joint regression forest (S-PRF) model to automatically digitize CMF landmarks. In this model, a regression voting strategy is first adopted to localize each landmark by aggregating evidences from context locations, thus potentially relieving the problem caused by image artifacts near the landmark. Second, CBCT image segmentation is utilized to remove uninformative voxels caused by morphological variations across patients. Third, a partially-joint model is further proposed to separately localize landmarks based on the coherence of landmark positions to improve the digitization reliability. In addition, we propose a fast vector quantization method to extract high-level multiscale statistical features to describe a voxel's appearance, which has low dimensionality, high efficiency, and is also invariant to the local inhomogeneity caused by artifacts.
Results: Mean digitization errors for 15 landmarks, in comparison to the ground truth, are all less than 2 mm.
Conclusion: Our model has addressed challenges of both interpatient morphological variations and imaging artifacts. Experiments on a CBCT dataset show that our approach achieves clinically acceptable accuracy for landmark digitalization.
Significance: Our automatic landmark digitization method can be used clinically to reduce the labor cost and also improve digitalization consistency.
Figures
References
-
- Donner R, Micušık B, Langs G, Bischof H. Sparse mrf appearance models for fast anatomical structur. localisation. Proc. BMVC. 2007
-
- Donner R, Langs G, Mičušik B, Bischof H. Generalized sparse mrf appearance models. Image and Vision Computing. 2010;28(6):1031–1038.
-
- Nowinski WL, Thirunavuukarasuu A. Atlas-assisted localization analysis of functional images. Medical Image Analysis. 2001;5(3):207–220. - PubMed
-
- Yelnik J, Damier P, Demeret S, Gervais D, Bardinet E, Bejjani B-P, François C, Houeto J-L, Arnulf I, Dormont D, et al. Localization of stimulating electrodes in patients with parkinson disease by using a three-dimensional atlas-magnetic resonance imaging coregistration method. Journal of neurosurgery. 2003;99(1):89–99. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
