

A randomized controlled trial of negative co-payments: the CHORD trial
- PMID: 26625506
- PMCID: PMC6171502
A randomized controlled trial of negative co-payments: the CHORD trial
Abstract
Objectives: Value-based insurance designs are being widely used. We undertook this study to examine whether a financial incentive that lowered co-payments for blood pressure medications below $0 improved blood pressure control among patients with poorly controlled hypertension.
Study design: Randomized controlled trial.
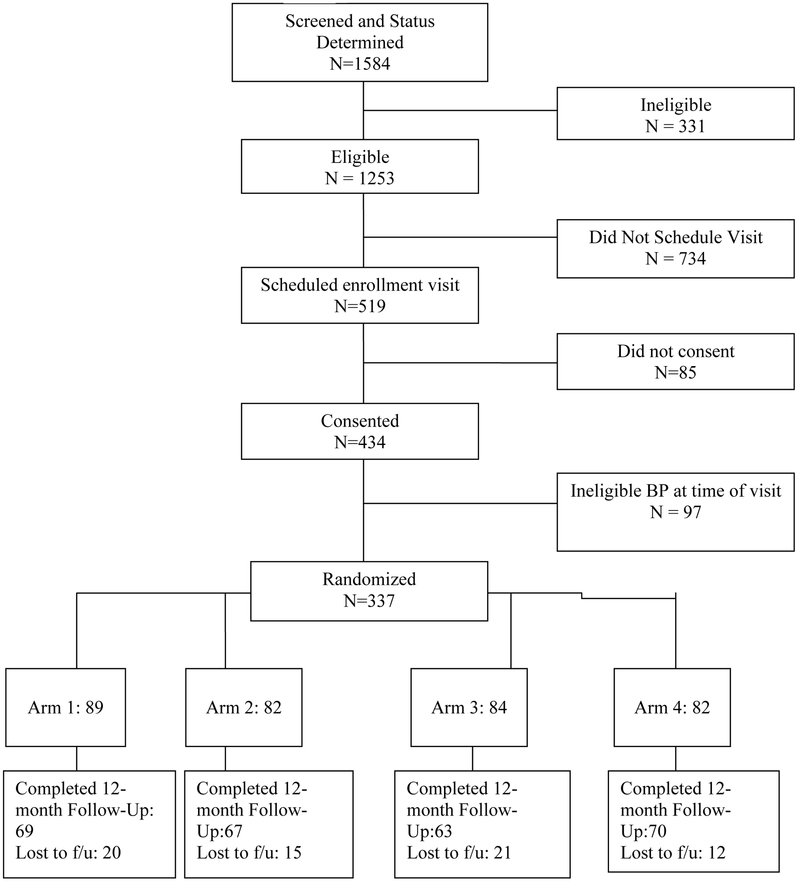
Methods: Participants from 3 Pennsylvania hospitals (n = 337) were randomly assigned to: a) be paid $8 per medication per month for filling blood pressure prescriptions, b) a computerized behavioral intervention (CBI), c) both payment and CBI, or d) usual care. The primary outcome was change in blood pressure between baseline and 12 months post enrollment. We also measured adherence using the medication possession ratio in a subset of participants.
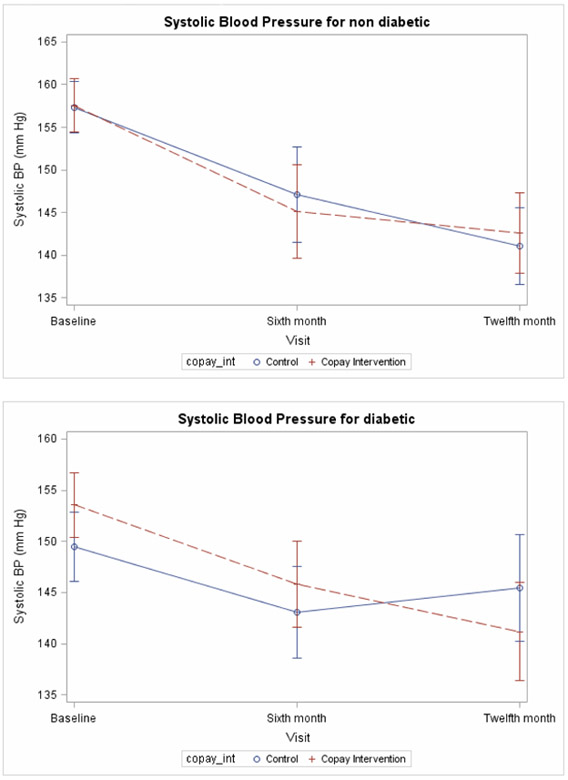
Results: There were no significant interactions between the incentive and the CBI interventions. There were no significant changes in medication possession ratio in the treatment group. Blood pressure decreased among all participants, but to a similar degree between the financial incentive and control groups. Systolic blood pressure (SBP) dropped 13.7 mm Hg for the incentive group versus 10.0 mm Hg for the control group (difference = –3.7; 95% CI, –9.0 to 1.6; P = .17). The proportion of patients with blood pressure under control 12 months post enrollment was 35.6% of the incentive group versus 27.7% of the control group (odds ratio, 1.4; 95% CI, 0.8-2.5; P = .19). Diabetics in the incentive group had an average drop in SBP of 12.7 mm Hg between baseline and 12 months compared with 4.0 mm Hg in the control group (P = .02). Patients in the incentive group without diabetes experienced average SBP reductions of 15.0 mm Hg, compared with 16.3 mm Hg for control group nondiabetics (P = .71).
Conclusions: Among patients with poorly controlled blood pressure, financial incentives—as implemented in this trial—did not improve blood pressure control or adherence except among patients with diabetes.
Figures
References
-
- Ho PM, Spertus JA, Masoudi FA, et al. Impact of medication therapy discontinuation on mortality after myocardial infarction. Arch Intern Med 2006;166:1842–7. - PubMed
-
- Osterberg L, Blaschke T. Adherence to medication. N Engl J Med 2005;353:487–97. - PubMed
-
- Jackevicius CA, Mamdani M, Tu JV. Adherence with statin therapy in elderly patients with and without acute coronary syndromes. JAMA : the journal of the American Medical Association 2002;288:462–7. - PubMed
-
- Haynes RB. Improving Patient Adherence: State of the art, with a special focus on medication taking for cardiovascular disorders In: Burke LE, Ockene IS, eds. Compliance in Healthcare and Research. Armonk, NY: Futura Publishing Company, Inc.; 2001:3–21.
-
- Ho PM, Rumsfeld JS, Masoudi FA, et al. Effect of medication nonadherence on hospitalization and mortality among patients with diabetes mellitus. Arch Intern Med 2006;166:1836–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical