

Improvement in Renal Function and Reduction in Serum Uric Acid with Intensive Statin Therapy in Older Patients: A Post Hoc Analysis of the SAGE Trial
- PMID: 26625880
- PMCID: PMC4676790
- DOI: 10.1007/s40266-015-0328-z
Improvement in Renal Function and Reduction in Serum Uric Acid with Intensive Statin Therapy in Older Patients: A Post Hoc Analysis of the SAGE Trial
Abstract
Background: Improvement in renal function and decreases in serum uric acid (SUA) have been reported following prolonged high-intensity statin (HMG-CoA reductase inhibitor) therapy. This post hoc analysis of the SAGE trial examined the effect of intensive versus less intensive statin therapy on renal function, safety, and laboratory parameters, including SUA, in elderly coronary artery disease (CAD) patients (65-85 years) with or without chronic kidney disease (CKD).
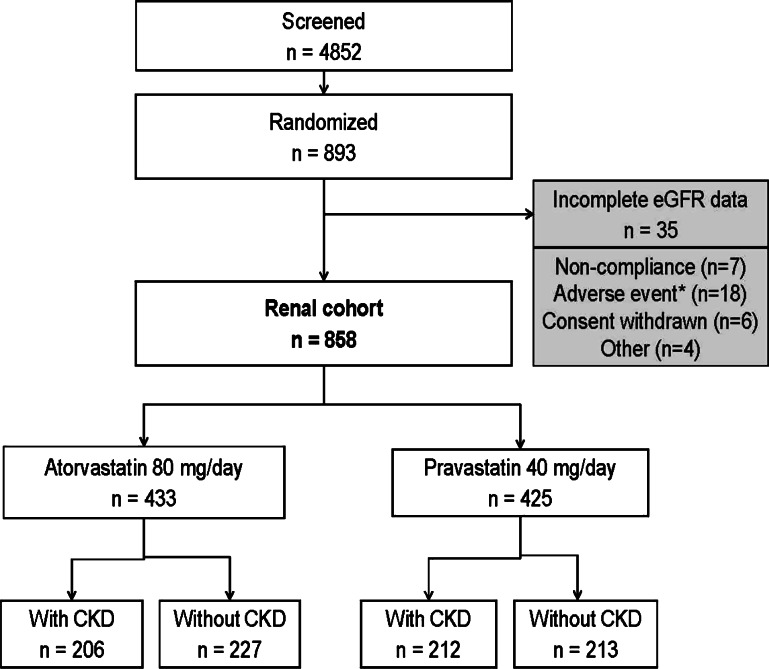
Methods: Patients were randomized to atorvastatin 80 mg/day or pravastatin 40 mg/day and treated for 12 months. Patients were stratified using Modification of Diet in Renal Disease (MDRD) estimated glomerular filtration rates (eGFRs) in CKD (eGFR <60 mL/min/1.73 m(2)) and non-CKD populations.
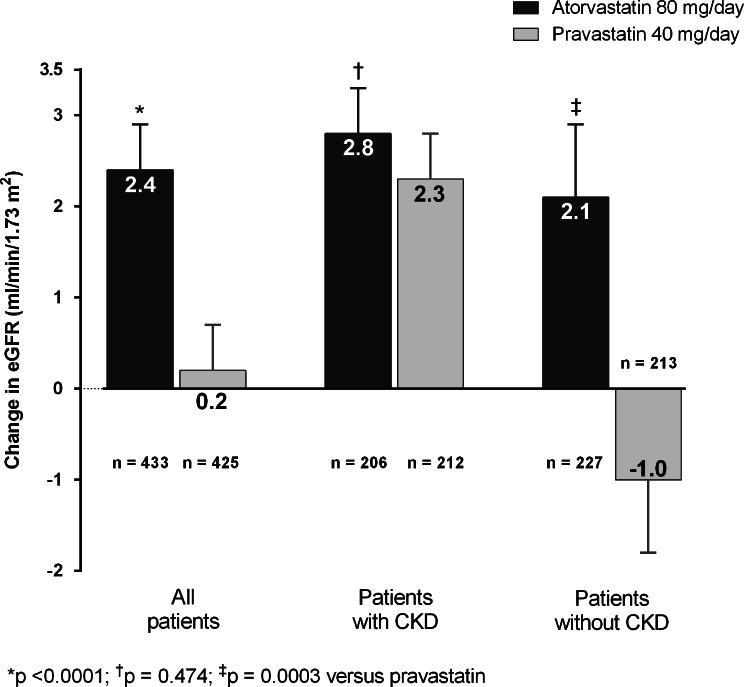
Results: Of the 893 patients randomized, 858 had complete renal data and 418 of 858 (49%) had CKD (99% Stage 3). Over 12 months, eGFR increased with atorvastatin and remained stable with pravastatin (+2.38 vs. +0.18 mL/min/1.73 m(2), respectively; p < 0.0001). MDRD eGFR improved significantly in both CKD treatment arms; however, the increased eGFR in patients without CKD was significantly greater with atorvastatin (+2.08 mL/min/1.73 m(2)) than with pravastatin (-1.04 mL/min/1.73 m(2)). Modest reductions in SUA were observed in both treatment arms, but a greater fall occurred with atorvastatin than with pravastatin (-0.52 vs. -0.09 mg/dL, p < 0.0001). Change in SUA correlated negatively with changes in eGFR and positively with changes in low-density lipoprotein cholesterol. Reports of myalgia were rare (3.6% CKD; 5.7% non-CKD), and there were no episodes of rhabdomyolysis. Elevated serum alanine and aspartate transaminase to >3 times the upper limit of normal occurred in 4.4% of atorvastatin- and 0.2% of pravastatin-treated patients.
Conclusion: Intensive management of dyslipidemia in older patients with stable coronary heart disease may have beneficial effects on renal function and SUA.
Figures

References
-
- Athyros VG, Elisaf M, Papageorgiou AA, Symeonidis AN, Pehlivanidis AN, Bouloukos VI, et al. Effect of statins versus untreated dyslipidemia on serum uric acid levels in patients with coronary heart disease: a subgroup analysis of the GREek Atorvastatin and Coronary-heart-disease Evaluation (GREACE) study. Am J Kidney Dis. 2004;43(4):589–599. doi: 10.1053/j.ajkd.2003.12.023. - DOI - PubMed
-
- Rahman M, Baimbridge C, Davis BR, Barzilay J, Basile JN, Henriquez MA, et al. Progression of kidney disease in moderately hypercholesterolemic, hypertensive patients randomized to pravastatin versus usual care: a report from the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) Am J Kidney Dis. 2008;52(3):412–424. doi: 10.1053/j.ajkd.2008.05.027. - DOI - PMC - PubMed
-
- Shepherd J, Kastelein JJ, Bittner V, Deedwania P, Breazna A, Dobson S, et al. Effect of intensive lipid lowering with atorvastatin on renal function in patients with coronary heart disease: the Treating to New Targets (TNT) study. Clin J Am Soc Nephrol. 2007;2(6):1131–1139. doi: 10.2215/CJN.04371206. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
