

Invasive meningococcal disease in England: assessing disease burden through linkage of multiple national data sources
- PMID: 26626321
- PMCID: PMC4667514
- DOI: 10.1186/s12879-015-1247-7
Invasive meningococcal disease in England: assessing disease burden through linkage of multiple national data sources
Abstract
Background: In England, Public Health England conducts enhanced surveillance of invasive meningococcal disease (IMD). The continuing decline in reported IMD cases has raised concerns that the MRU may be underestimating true IMD incidence.
Methods: We linked five national datasets to estimate disease burden over five years, including PHE Meningococcal Reference Unit (MRU) confirmations, hospital episode statistics (HES), electronic reports of significant infections by National Health Service (NHS) Hospitals, death registrations and private laboratory reports.
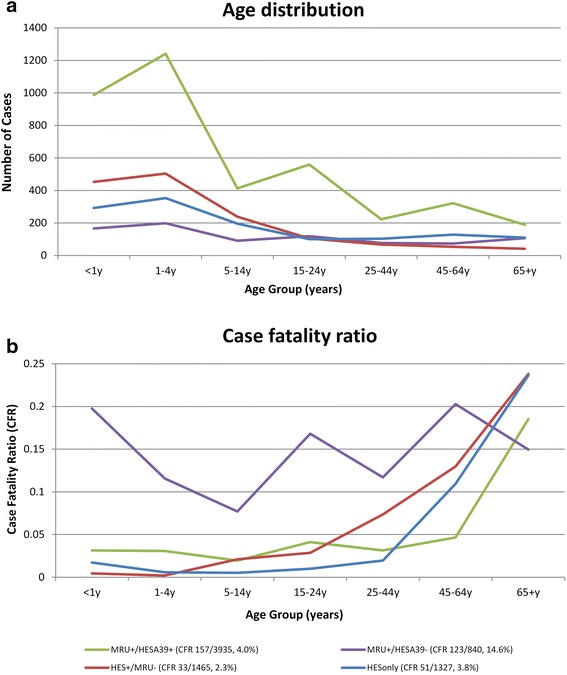
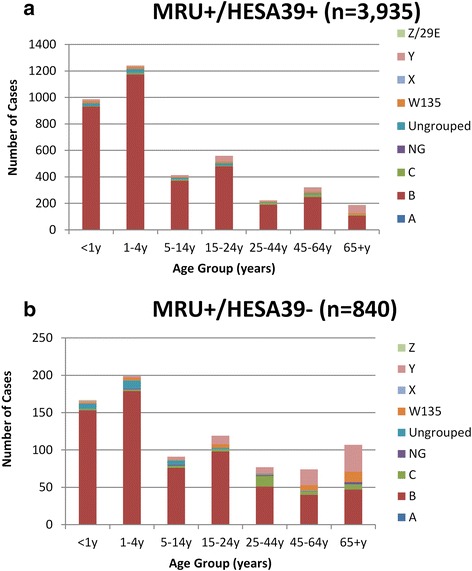
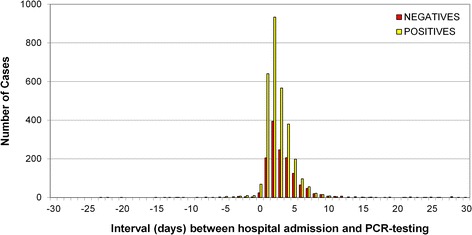
Results: During 2007-11, MRU confirmed 5115 IMD cases and 4275 (84%) matched to HES, including 3935 (92%) with A39* (meningococcal disease) and 340 (8%) with G00* (bacterial meningo-encephalitis) ICD-10 codes. An additional 2792 hospitalised cases with an A39* code were identified in HES. Of these, 1465 (52%) matched to one of 53,806 samples tested PCR-negative for IMD by MRU and only 73 of the remaining 1327 hospitalised A39* cases were confirmed locally or by a private laboratory. The characteristics of hospitalised cases without laboratory confirmation were similar to PCR-negative than PCR-positive IMD cases.
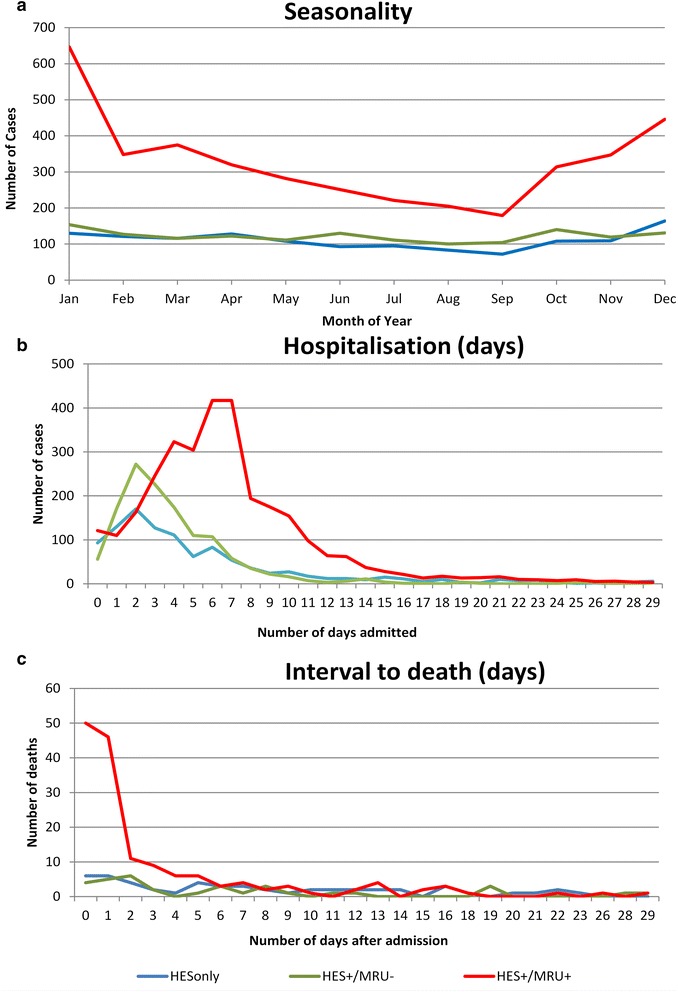
Conclusions: Interrogation of multiple national data sources identified very few laboratory confirmations in addition to the MRU-confirmed cases. The large number of unconfirmed and PCR-negative cases in HES suggests increased awareness among clinicians with low thresholds for hospitalising patients with suspected IMD.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
