

A first-in-human phase 1 study of ACE910, a novel factor VIII-mimetic bispecific antibody, in healthy subjects
- PMID: 26626991
- PMCID: PMC4817308
- DOI: 10.1182/blood-2015-06-650226
A first-in-human phase 1 study of ACE910, a novel factor VIII-mimetic bispecific antibody, in healthy subjects
Abstract
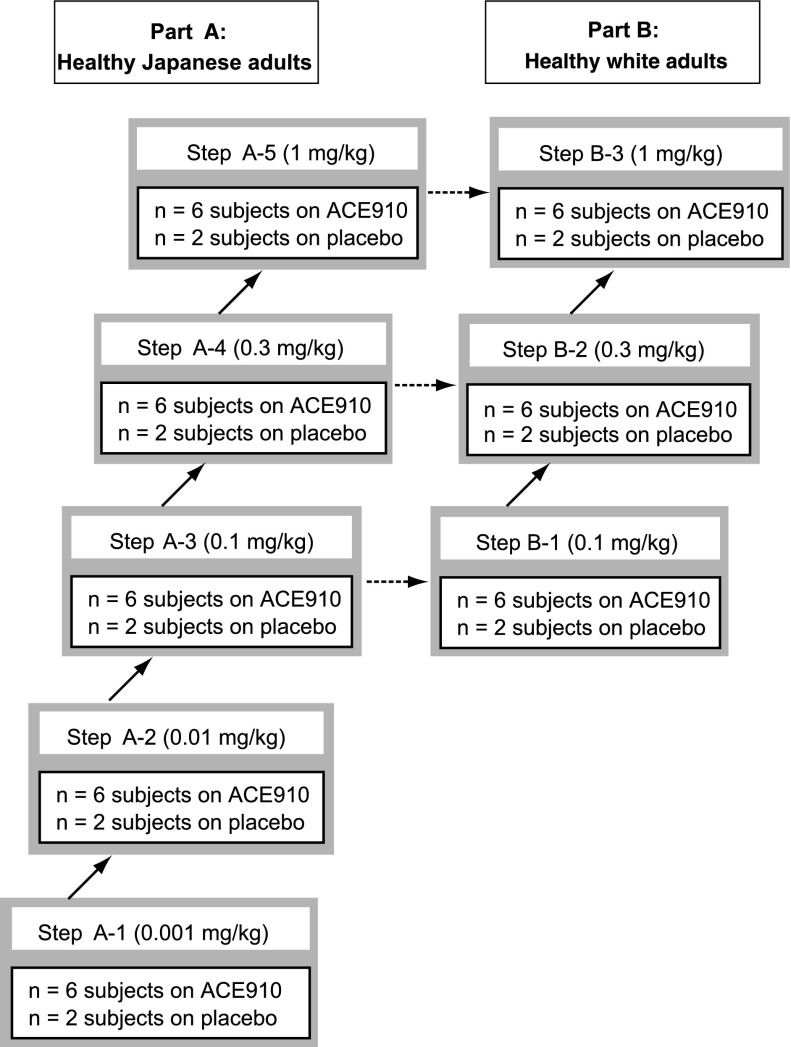
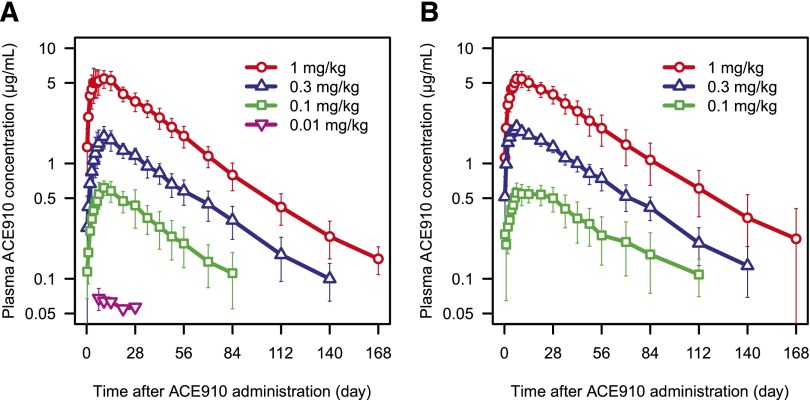
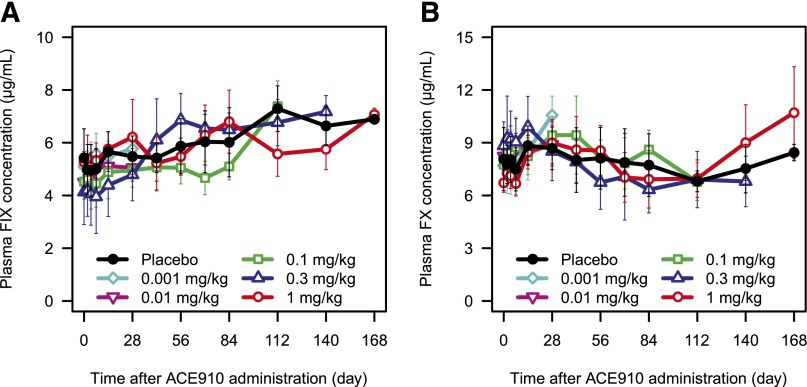
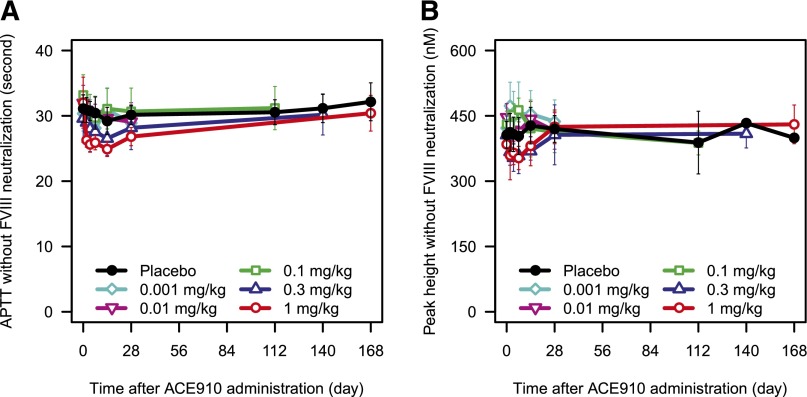
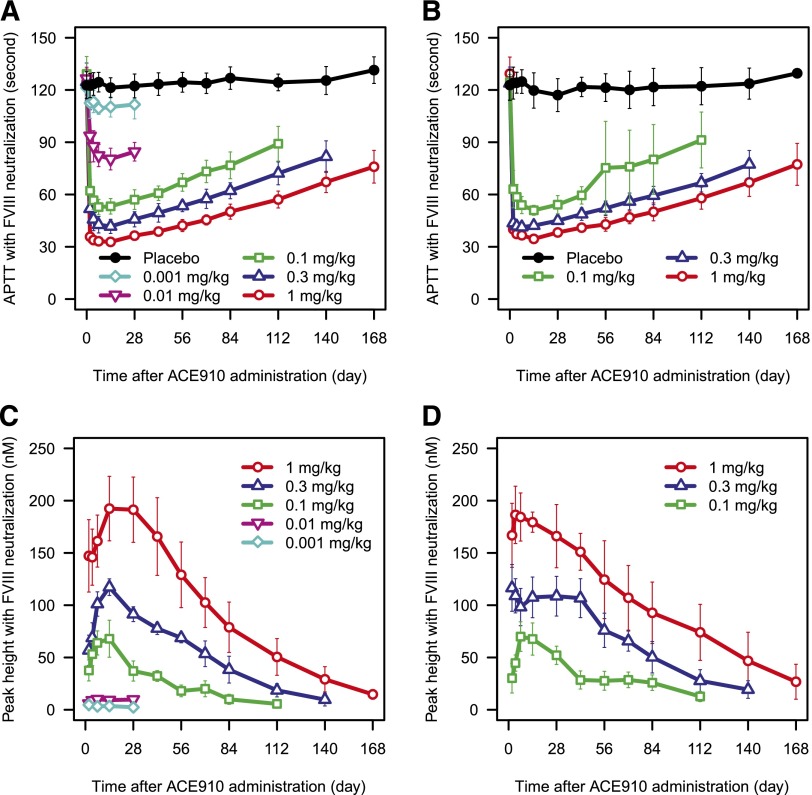
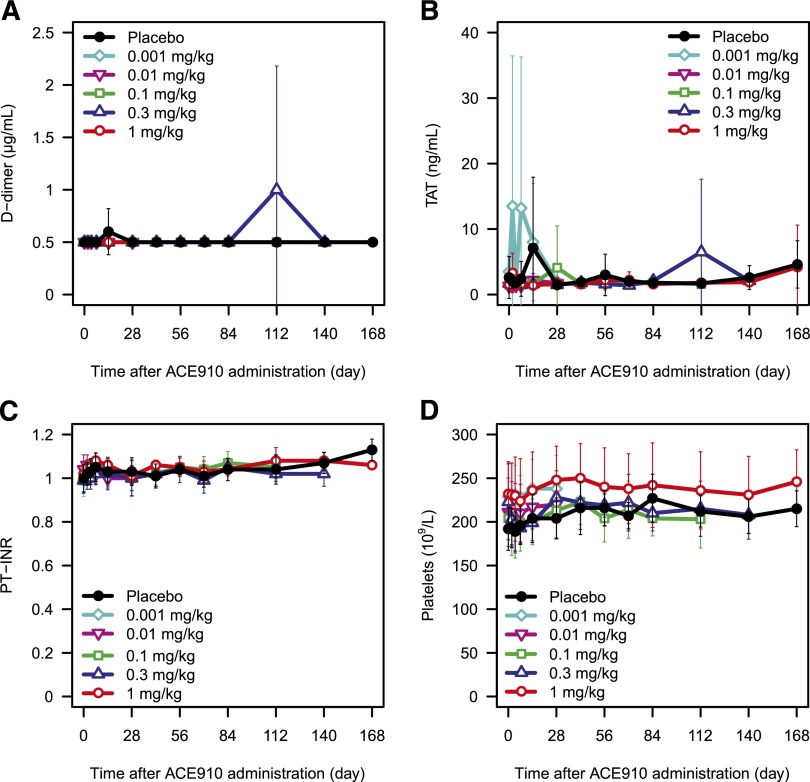
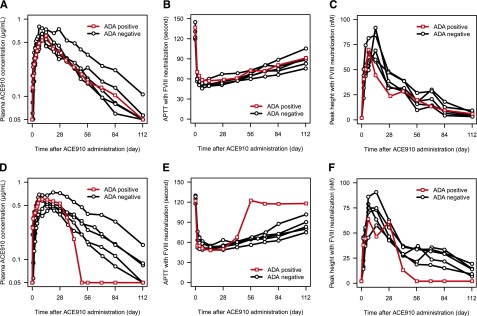
ACE910 is a recombinant humanized bispecific antibody that binds to activated factor IX and factor X and mimics the cofactor function of factor VIII (FVIII). This first-in-human study examined the safety, tolerability, pharmacokinetics (PK), and pharmacodynamics (PD) of ACE910 in healthy male adults. A total of 40 Japanese and 24 white subjects were randomized to receive a single subcutaneous injection of ACE910 (Japanese: 0.001, 0.01, 0.1, 0.3, or 1 mg/kg; white: 0.1, 0.3, or 1 mg/kg; n = 6 per dose group) or placebo (n = 2 per dose group). ACE910 exhibited a linear PK profile and had a half-life of ∼4 to 5 weeks. In FVIII-neutralized plasma, ACE910 shortened activated partial thromboplastin time and increased peak height of thrombin generation in a dose-dependent manner. All adverse events were nonserious and did not lead to any subject's withdrawal. Neither clinical findings nor laboratory abnormalities indicating hypercoagulability were observed. Two of 48 subjects receiving ACE910 (1 Japanese and 1 white) were positive for anti-ACE910 antibodies (anti-drug antibodies [ADAs]). One subject tested positive for ADAs both before and after ACE910 administration, whereas the other became ADA positive after receiving ACE910. The PK and PD profiles of ACE910 were similar in healthy Japanese and white subjects and suggest that ACE910 will be an effective and convenient prophylactic treatment of hemophilia A. This trial was registered at www.clinicaltrials.jp as #JapicCTI-121934.
© 2016 by The American Society of Hematology.
Figures
Comment in
-
Hemophilia A treatment: disruptive technology ahead.Blood. 2016 Mar 31;127(13):1623-4. doi: 10.1182/blood-2016-01-691469. Blood. 2016. PMID: 27034415
References
-
- Srivastava A, Brewer AK, Mauser-Bunschoten EP, et al. Treatment Guidelines Working Group on Behalf of the World Federation of Hemophilia. Guidelines for the management of hemophilia. Haemophilia. 2013;19(1):e1–e47. - PubMed
-
- Löfqvist T, Nilsson IM, Berntorp E, Pettersson H. Haemophilia prophylaxis in young patients – a long-term follow-up. J Intern Med. 1997;241(5):395–400. - PubMed
-
- Manco-Johnson MJ, Abshire TC, Shapiro AD, et al. Prophylaxis versus episodic treatment to prevent joint disease in boys with severe hemophilia. N Engl J Med. 2007;357(6):535–544. - PubMed
-
- Geraghty S, Dunkley T, Harrington C, Lindvall K, Maahs J, Sek J. Practice patterns in haemophilia A therapy – global progress towards optimal care. Haemophilia. 2006;12(1):75–81. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
