

Survival Impact of Increasing Time to Treatment Initiation for Patients With Head and Neck Cancer in the United States
- PMID: 26628469
- PMCID: PMC4858932
- DOI: 10.1200/JCO.2015.61.5906
Survival Impact of Increasing Time to Treatment Initiation for Patients With Head and Neck Cancer in the United States
Abstract
Purpose: To estimate the overall survival (OS) impact from increasing time to treatment initiation (TTI) for patients with head and neck squamous cell carcinoma (HNSCC).
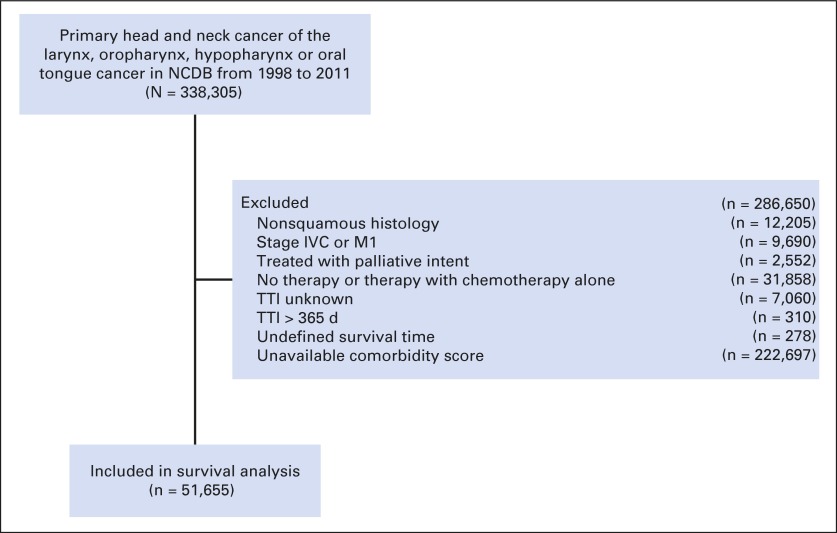
Methods: Using the National Cancer Data Base (NCDB), we examined patients who received curative therapy for the following sites: oral tongue, oropharynx, larynx, and hypopharynx. TTI was the number of days from diagnosis to initiation of curative treatment. The effect of TTI on OS was determined by using Cox regression models (MVA). Recursive partitioning analysis (RPA) identified TTI thresholds via conditional inference trees to estimate the greatest differences in OS on the basis of randomly selected training and validation sets, and repeated this 1,000 times to ensure robustness of TTI thresholds.
Results: A total of 51,655 patients were included. On MVA, TTI of 61 to 90 days versus less than 30 days (hazard ratio [HR], 1.13; 95% CI, 1.08 to 1.19) independently increased mortality risk. TTI of 67 days appeared as the optimal threshold on the training RPA, statistical significance was confirmed in the validation set (P < .001), and the 67-day TTI was the optimal threshold in 54% of repeated simulations. Overall, 96% of simulations validated two optimal TTI thresholds, with ranges of 46 to 52 days and 62 to 67 days. The median OS for TTI of 46 to 52 days or fewer versus 53 to 67 days versus greater than 67 days was 71.9 months (95% CI, 70.3 to 73.5 months) versus 61 months (95% CI, 57 to 66.1 months) versus 46.6 months (95% CI, 42.8 to 50.7 months), respectively (P < .001). In the most recent year with available data (2011), 25% of patients had TTI of greater than 46 days.
Conclusion: TTI independently affects survival. One in four patients experienced treatment delay. TTI of greater than 46 to 52 days introduced an increased risk of death that was most consistently detrimental beyond 60 days. Prolonged TTI is currently affecting survival.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures




Comment in
-
Looking Beyond the Numbers: Highlighting the Challenges of Population-Based Studies in Cancer Research.J Clin Oncol. 2016 Jul 1;34(19):2317-8. doi: 10.1200/JCO.2015.66.0894. Epub 2016 Apr 25. J Clin Oncol. 2016. PMID: 27114596 No abstract available.
-
Reply to P. Blanchard et al.J Clin Oncol. 2016 Jul 1;34(19):2318-9. doi: 10.1200/JCO.2016.67.2832. Epub 2016 Apr 25. J Clin Oncol. 2016. PMID: 27114603 No abstract available.
-
Head and neck surgery recommendations during the COVID-19 pandemic - Author's reply.Lancet Oncol. 2020 Sep;21(9):e417. doi: 10.1016/S1470-2045(20)30480-0. Lancet Oncol. 2020. PMID: 32888467 Free PMC article. No abstract available.
References
-
- Murphy CT, Galloway TJ, Handorf EA, et al. Increasing time to treatment initiation for head and neck cancer: An analysis of the National Cancer Database. Cancer. 2015;121:1204–1213. - PubMed
-
- Sher DJ, Neville BA, Chen AB, et al. Predictors of IMRT and conformal radiotherapy use in head and neck squamous cell carcinoma: A SEER-Medicare analysis. Int J Radiat Oncol Biol Phys. 2011;81:e197–e206. - PubMed
-
- Smith BD, Haffty BG, Wilson LD, et al. The future of radiation oncology in the United States from 2010 to 2020: Will supply keep pace with demand. J Clin Oncol. 2010;28:5160–5165. - PubMed
-
- Institute of Medicine Crossing the quality chasm: A new health system for the 21st century. http://www.iom.edu/Reports/2001/Crossing-the-Quality-Chasm-A-New-Health-....
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
