

Associations between exemption and survival outcomes in the UK's primary care pay-for-performance programme: a retrospective cohort study
- PMID: 26628553
- PMCID: PMC5013124
- DOI: 10.1136/bmjqs-2015-004602
Associations between exemption and survival outcomes in the UK's primary care pay-for-performance programme: a retrospective cohort study
Abstract
Objectives: The UK's Quality and Outcomes Framework permits practices to exempt patients from financially-incentivised performance targets. To better understand the determinants and consequences of being exempted from the framework, we investigated the associations between exception reporting, patient characteristics and mortality. We also quantified the proportion of exempted patients that met quality targets for a tracer condition (diabetes).
Design: Retrospective longitudinal study, using individual patient data from the Clinical Practice Research Datalink.
Setting: 644 general practices, 2006/7 to 2011/12.
Participants: Patients registered with study practices for at least one year over the study period, with at least one condition of interest (2 460 341 in total).
Main outcome measures: Exception reporting rates by reason (clinical contraindication, patient dissent); all-cause mortality in year following exemption. Analyses with logistic and Cox proportional-hazards regressions, respectively.
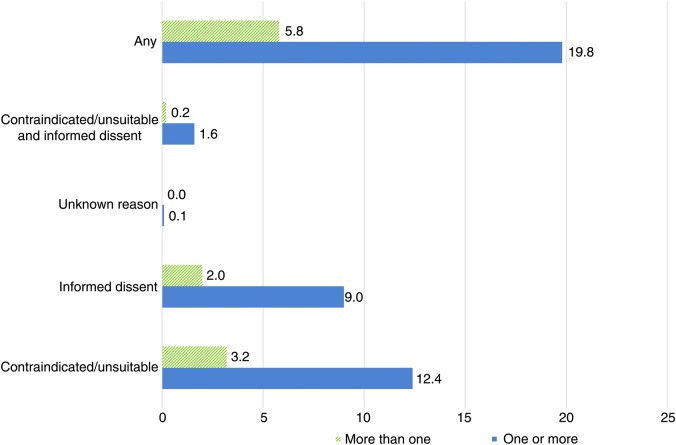
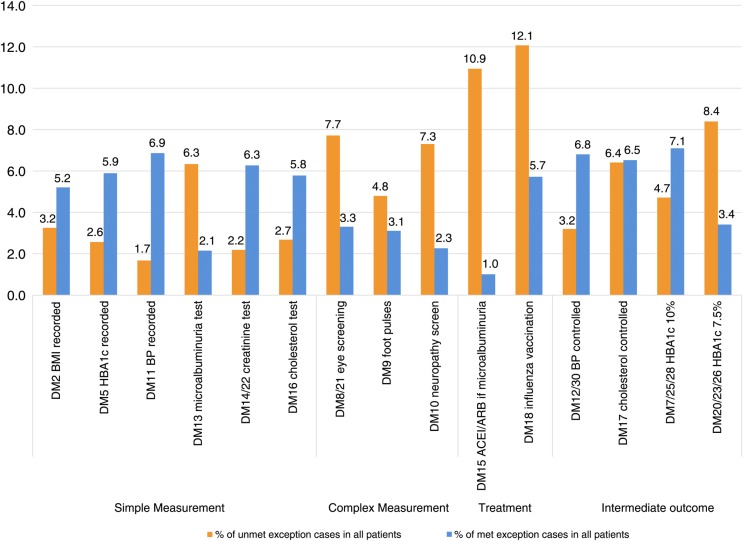
Results: The odds of being exempted increased with age, deprivation and multimorbidity. Men were more likely to be exempted but this was largely attributable to higher prevalence of conditions with high exemption rates. Modest associations remained, with women more likely to be exempted due to clinical contraindication (OR 0.90, 99% CI 0.88 to 0.92) and men more likely to be exempted due to informed dissent (OR 1.08, 99% CI 1.06 to 1.10). More deprived areas (both for practice location and patient residence) were non-linearly associated with higher exception rates, after controlling for comorbidities and other covariates, with stronger associations for clinical contraindication. Compared with patients with a single condition, odds ratios for patients with two, three, or four or more conditions were respectively 4.28 (99% CI 4.18 to 4.38), 16.32 (99% CI 15.82 to 16.83) and 68.69 (99% CI 66.12 to 71.37) for contraindication, and 2.68 (99% CI 2.63 to 2.74), 4.02 (99% CI 3.91 to 4.13) and 5.17 (99% CI 5.00 to 5.35) for informed dissent. Exempted patients had a higher adjusted risk of death in the following year than non-exempted patients, regardless of whether this exemption was for contraindication (hazard ratio 1.37, 99% CI 1.33 to 1.40) or for informed dissent (1.20, 99% CI 1.17 to 1.24). On average, quality standards were met for 48% of exempted patients in the diabetes domain, but there was wide variation across indicators (ranging from 8 to 80%).
Conclusions: Older, multimorbid and more deprived patients are more likely to be exempted from the scheme. Exception reported patients are more likely to die in the following year, whether they are exempted by the practice for a contraindication or by themselves through informed dissent. Further research is needed to understand the relationship between exception reporting and patient outcomes.
Keywords: Diabetes mellitus; Financial incentives; General practice; Health services research; Pay for performance.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
Comment in
-
Should doctors be able to exclude patients from pay-for-performance schemes?BMJ Qual Saf. 2016 Sep;25(9):653-6. doi: 10.1136/bmjqs-2015-005003. Epub 2015 Dec 30. BMJ Qual Saf. 2016. PMID: 26717988 No abstract available.
References
-
- Centers for Medicare & Medicaid Services (CMS), HHS. Medicare program; hospital inpatient value-based purchasing program. Final rule. Fed Regist 2011;76:26490–547. - PubMed
-
- Centers for Medicare & Medicaid Services (CMS), HHS. Medicare program; hospital inpatient prospective payment systems for acute care hospitals and the long-term care hospital prospective payment system and fiscal year 2015 rates; quality reporting requirements for specific providers; reasonable compensation equivalents for physician services in excluded hospitals and certain teaching hospitals; provider administrative appeals and judicial review; enforcement provisions for organ transplant centers; and electronic health record (EHR) incentive program. Final rule. Fed Regist 2014;79:49853–50536. - PubMed
-
- Australia M. Practice incentives program. Sydney: Australian Government, 2011.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous