

The role of B-cell receptor inhibitors in the treatment of patients with chronic lymphocytic leukemia
- PMID: 26628631
- PMCID: PMC4666325
- DOI: 10.3324/haematol.2014.119123
The role of B-cell receptor inhibitors in the treatment of patients with chronic lymphocytic leukemia
Abstract
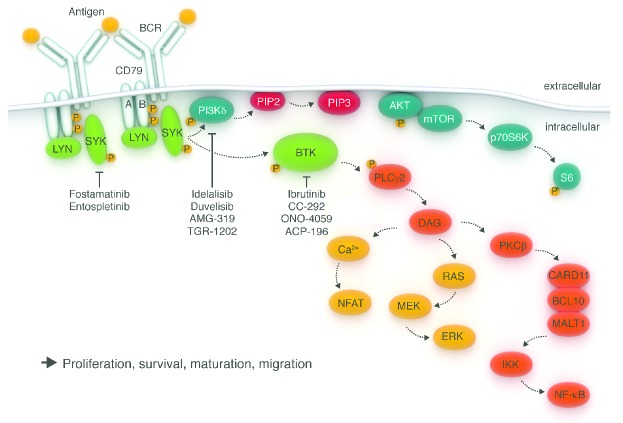
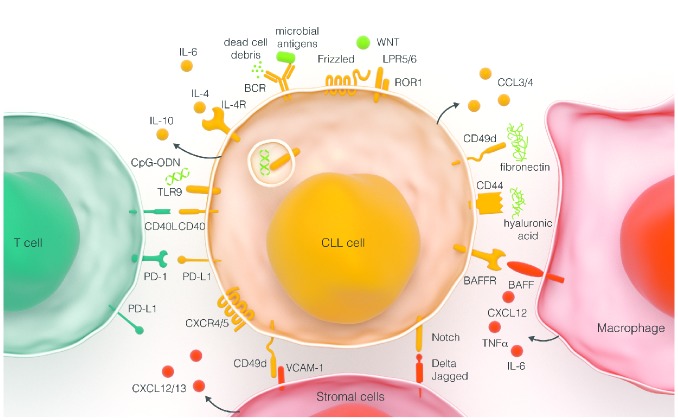
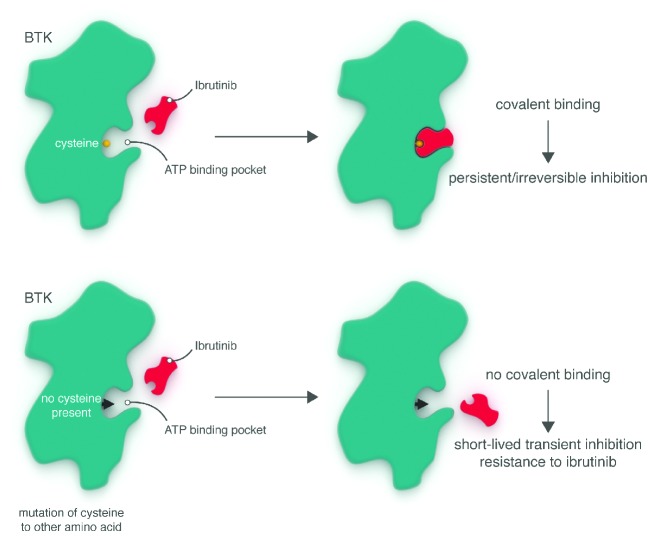
Chronic lymphocytic leukemia is a malignancy of mature auto-reactive B cells. Genetic and functional studies implicate B-cell receptor signaling as a pivotal pathway in its pathogenesis. Full B-cell receptor activation requires tumor-microenvironment interactions in lymphoid tissues. Spleen tyrosine kinase, Bruton's tyrosine kinase, and the phosphatidylinositol 3-kinase (PI3K) δ isoform are essential for B-cell receptor signal transduction but also mediate the effect of other pathways engaged in chronic lymphocytic leukemia cells in the tissue-microenvironment. Orally bioavailable inhibitors of spleen tyrosine kinase, Bruton's tyrosine kinase, or PI3Kδ, induce high rates of durable responses. Ibrutinib, a covalent inhibitor of Bruton's tyrosine kinase, and idelalisib, a selective inhibitor of PI3Kδ, have obtained regulatory approval in chronic lymphocytic leukemia. Ibrutinib and idelalisib are active in patients with high-risk features, achieving superior disease control in difficult-to-treat patients than prior best therapy, making them the preferred agents for chronic lymphocytic leukemia with TP53 aberrations and for patients resistant to chemoimmunotherapy. In randomized trials, both ibrutinib, versus ofatumumab, and idelalisib in combination with rituximab, versus placebo with rituximab improved survival in relapsed/refractory chronic lymphocytic leukemia. Responses to B-cell receptor inhibitors are mostly partial, and within clinical trials treatment is continued until progression or occurrence of intolerable side effects. Ibrutinib and idelalisib are, overall, well tolerated; notable adverse events include increased bruising and incidence of atrial fibrillation on ibrutinib and colitis, pneumonitis and transaminase elevations on idelalisib. Randomized trials investigate the role of B-cell receptor inhibitors in first-line therapy and the benefit of combinations. This review discusses the biological basis for targeted therapy of chronic lymphocytic leukemia with B-cell receptor inhibitors, and summarizes the clinical experience with these agents.
Copyright© Ferrata Storti Foundation.
Figures
References
-
- Hallek M, Cheson BD, Catovsky D, et al. Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute-Working Group 1996 guidelines. Blood. 2008;111(12): 5446–5456. - PMC - PubMed
-
- Wierda WG, O’Brien S, Wang X, et al. Prognostic nomogram and index for overall survival in previously untreated patients with chronic lymphocytic leukemia. Blood. 2007;109(11):4679–4685. - PubMed
-
- Dohner H, Stilgenbauer S, Benner A, et al. Genomic aberrations and survival in chronic lymphocytic leukemia. N Engl J Med. 2000;343(26):1910–1916. - PubMed
-
- Orchard JA, Ibbotson RE, Davis Z, et al. ZAP-70 expression and prognosis in chronic lymphocytic leukaemia. Lancet. 2004;363(9403):105–111. - PubMed
-
- Goede V, Fischer K, Busch R, et al. Obinutuzumab plus chlorambucil in patients with CLL and coexisting conditions. N Engl J Med. 2014;370(12):1101–1110. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
