

Physician preferences for bone metastasis drug therapy in Canada
- PMID: 26628874
- PMCID: PMC4608407
- DOI: 10.3747/co.22.2380
Physician preferences for bone metastasis drug therapy in Canada
Abstract
Background: Currently in Canada, several bone-targeted agents (btas) with varying characteristics are available for the prevention of skeletal-related events (sres) in patients with bone metastasis secondary to solid tumours. In the present study, we evaluated the preferences of physicians in Canada for the various attributes of the available btas.
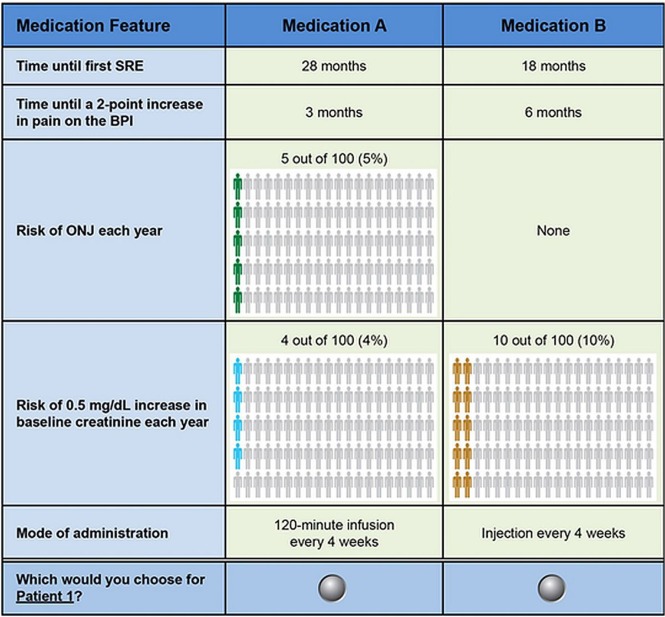
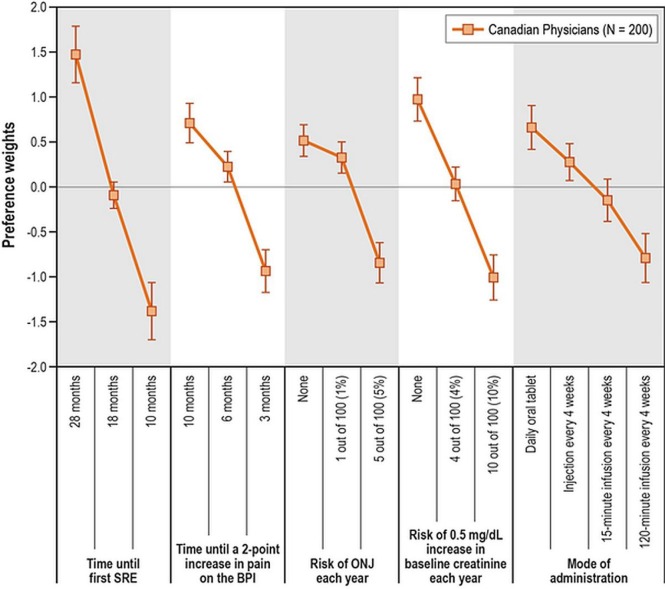
Methods: Physicians treating patients with bone metastasis from solid tumours were invited to complete an online discrete-choice experiment. Respondents were asked to choose between pairs of hypothetical medications for virtual patients. Each hypothetical medication was described based on predefined key attributes: time until first sre, time until worsening of pain, medication-related annual risk of osteonecrosis of the jaw (onj), medication-related annual risk of renal impairment, and mode of administration. A random-parameters logit model was used to analyze the choices between hypothetical medications and thus infer physician preferences for medication attributes.
Results: Responses from the 200 physicians who completed the discrete-choice experiment suggested that months until first sre, risk of renal impairment, and months until worsening of pain were considered the most important attributes affecting choice of bta. The annual risk of onj was considered the least important attribute.
Conclusions: When making treatment decisions about the choice of bta for patients with bone metastasis from solid tumours, delaying sres and worsening of pain, and reducing the risk of renal impairment are primary considerations for physicians in Canada.
Keywords: Bone metastases; bone-targeted agents; conjoint analysis; discrete-choice experiments; physician preferences; skeletal-related events.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
