

Third-line antiretroviral therapy in Africa: effectiveness in a Southern African retrospective cohort study
- PMID: 26628902
- PMCID: PMC4666151
- DOI: 10.1186/s12981-015-0081-8
Third-line antiretroviral therapy in Africa: effectiveness in a Southern African retrospective cohort study
Abstract
Background: An increasing number of patients in Africa are experiencing virologic failure on second-line antiretroviral therapy (ART) and those who develop resistance to protease inhibitors (PI) will require third-line ART, but no data on the outcomes of third-line are available from the region. We assessed the virologic outcomes and survival of patients started on salvage ART in a Southern African private sector disease management programme.
Methods: Retrospective observational cohort study with linkage to the national death register. Adults (≥18 years) who started salvage ART between July 2007 and December 2011 were included. Salvage ART was defined by inclusion of darunavir or tipranavir in an ART regimen after having failed another PI. For Kaplan-Meier (KM) analysis, patients were followed up until event, or censored at death (only for virologic outcomes), leaving the programme, or April 2014.
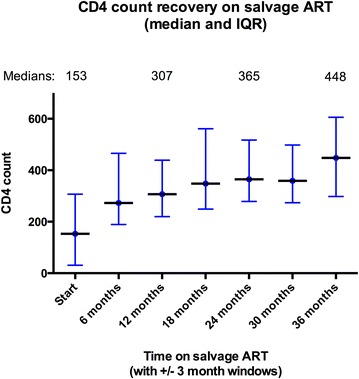
Results: 152 patients were included. Subtype was known for 113 patients: 111 (98 %) were infected with subtype C. All 152 had a genotype resistance test demonstrating major PI resistance mutations. Salvage drugs included were: darunavir/ritonavir (n = 149), tipranavir/ritonavir (n = 3), raltegravir (n = 58), and etravirine (n = 8). Median follow-up was 2.5 years (IQR = 1.5-3.3). 82.9 % achieved a viral load ≤400 copies/ml and 71.1 % ≤50 copies/ml. By the end of the study 17 (11.2 %) of the patients had died. The KM estimate of cumulative survival was 87.2 % at 2000 days.
Conclusions: Virologic suppression was comparable to that demonstrated in clinical trials and observational studies of salvage ART drugs conducted in other regions. Few deaths occurred during short term follow-up. Third-line regimens for patients with multidrug resistant subtype C HIV in Africa are virologically and clinically effective.
Keywords: Antiretroviral therapy; HIV; Human immunodeficiency virus; Salvage; Third-line; Virologic failure.
Figures

References
-
- Van Zyl GU, Liu TF, Claassen M, Engelbrecht S, de Oliveira T, Preiser W, Wood NT, Travers S, Shafer RW. Trends in genotypic HIV-1 antiretroviral resistance between 2006 and 2012 in South African patients receiving first- and second-line antiretroviral treatment regimens. PLoS One. 2013;8(6):e67188. doi: 10.1371/journal.pone.0067188. - DOI - PMC - PubMed
-
- Rawizza HE, Chaplin B, Meloni ST, Darin KM, Olaitan O, Scarsi KK, Onwuamah CK, Audu RA, Chebu PR, Imade GE, et al. Accumulation of protease mutations among patients failing second-line antiretroviral therapy and response to salvage therapy in Nigeria. PLoS One. 2013;8(9):e73582. doi: 10.1371/journal.pone.0073582. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
