

Pathophysiologic Response to Burns in the Elderly
- PMID: 26629550
- PMCID: PMC4634201
- DOI: 10.1016/j.ebiom.2015.07.040
Pathophysiologic Response to Burns in the Elderly
Abstract
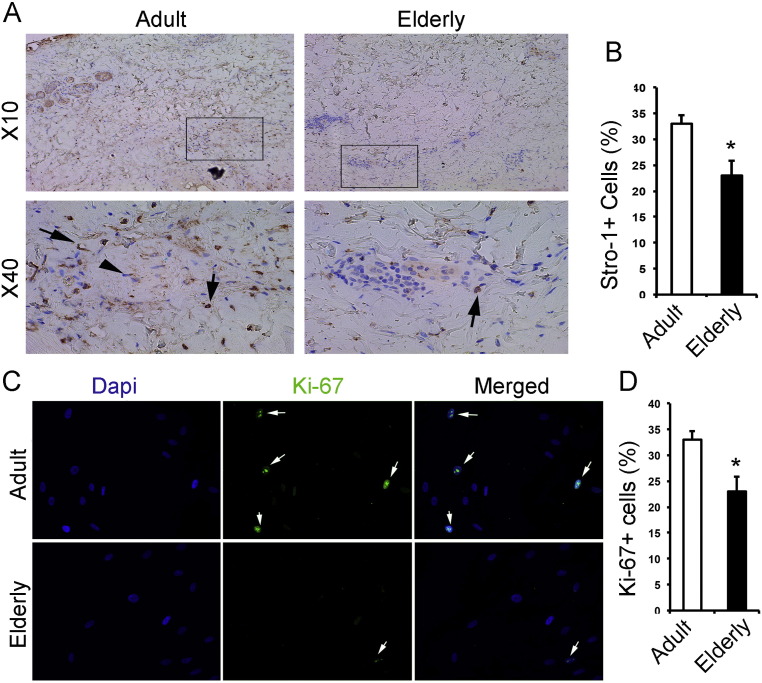
Over the last decades advancements have improved survival and outcomes of severely burned patients except one population, elderly. The Lethal Dose 50 (LD50) burn size in elderly has remained the same over the past three decades, and so has morbidity and mortality, despite the increased demand for elderly burn care. The objective of this study is to gain insights on why elderly burn patients have had such a poor outcome when compared to adult burn patients. The significance of this project is that to this date, burn care providers recognize the extreme poor outcome of elderly, but the reason remains unclear. In this prospective translational trial, we have determined clinical, metabolic, inflammatory, immune, and skin healing aspects. We found that elderly have a profound increased mortality, more premorbid conditions, and stay at the hospital for longer, p < 0.05. Interestingly, we could not find a higher incidence of infection or sepsis in elderly, p > 0.05, but a significant increased incidence of multi organ failure, p < 0.05. These clinical outcomes were associated with a delayed hypermetabolic response, increased hyperglycemic and hyperlipidemic responses, inversed inflammatory response, immune-compromisation and substantial delay in wound healing predominantly due to alteration in characteristics of progenitor cells, p < 0.05. In summary, elderly have substantially different responses to burns when compared to adults associated with increased morbidity and mortality. This study indicates that these responses are complex and not linear, requiring a multi-modal approach to improve the outcome of severely burned elderly.
Keywords: Burn; Elderly; Hypermetabolism; Inflammasome; Inflammation; Morbidity; Mortality; Pathophysiologic response; Skin healing; Stem cell.
Figures











Comment in
-
Response to Burns in the Elderly: What is Pathophysiology and What is Physiology?EBioMedicine. 2015 Sep 7;2(10):1314-5. doi: 10.1016/j.ebiom.2015.09.009. eCollection 2015 Oct. EBioMedicine. 2015. PMID: 26629525 Free PMC article. No abstract available.
References
-
- (WHO) OWH . 2002. A Graphical Overview of the Global Burden of Injuries. The Injury Chart Book. (Geneva)
-
- Albornoz C.R., Villegas J., Sylvester M., Pena V., Bravo I. Burns are more aggressive in the elderly: proportion of deep burn area/total burn area might have a role in mortality. Burns. 2011;37:1058–1061. - PubMed
-
- Amini Nik S., Ebrahim R.P., Van Dam K., Cassiman J.J., Tejpar S. TGF-beta modulates beta-catenin stability and signaling in mesenchymal proliferations. Exp. Cell Res. 2007;313:2887–2895. - PubMed
-
- Amini-Nik S., Glancy D., Boimer C., Whetstone H., Keller C., Alman B.A. Pax7 expressing cells contribute to dermal wound repair, regulating scar size through a beta-catenin mediated process. Stem Cells (Dayton, Ohio) 2011;29:1371–1379. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
