

Defining the Effect of the 16p11.2 Duplication on Cognition, Behavior, and Medical Comorbidities
- PMID: 26629640
- PMCID: PMC5894477
- DOI: 10.1001/jamapsychiatry.2015.2123
Defining the Effect of the 16p11.2 Duplication on Cognition, Behavior, and Medical Comorbidities
Abstract
Importance: The 16p11.2 BP4-BP5 duplication is the copy number variant most frequently associated with autism spectrum disorder (ASD), schizophrenia, and comorbidities such as decreased body mass index (BMI).
Objectives: To characterize the effects of the 16p11.2 duplication on cognitive, behavioral, medical, and anthropometric traits and to understand the specificity of these effects by systematically comparing results in duplication carriers and reciprocal deletion carriers, who are also at risk for ASD.
Design, setting, and participants: This international cohort study of 1006 study participants compared 270 duplication carriers with their 102 intrafamilial control individuals, 390 reciprocal deletion carriers, and 244 deletion controls from European and North American cohorts. Data were collected from August 1, 2010, to May 31, 2015 and analyzed from January 1 to August 14, 2015. Linear mixed models were used to estimate the effect of the duplication and deletion on clinical traits by comparison with noncarrier relatives.
Main outcomes and measures: Findings on the Full-Scale IQ (FSIQ), Nonverbal IQ, and Verbal IQ; the presence of ASD or other DSM-IV diagnoses; BMI; head circumference; and medical data.
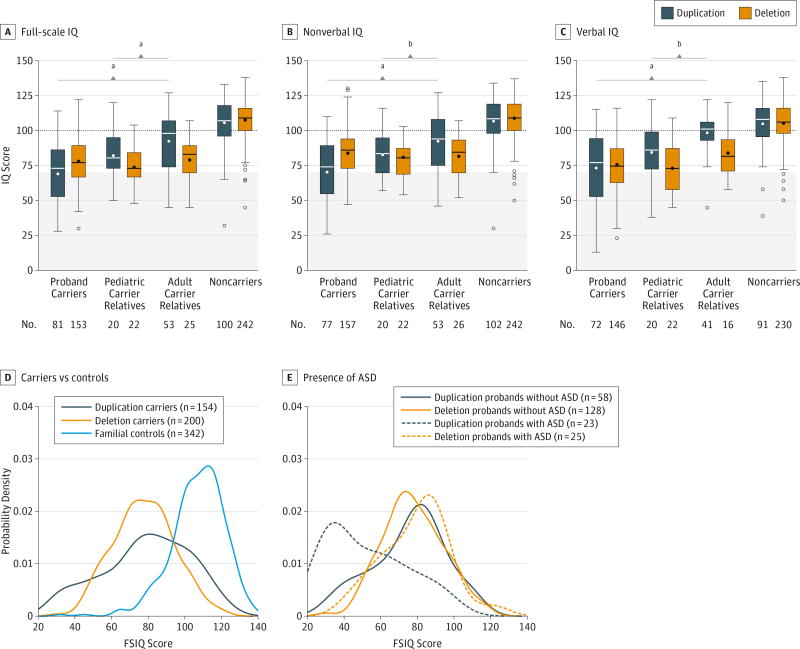
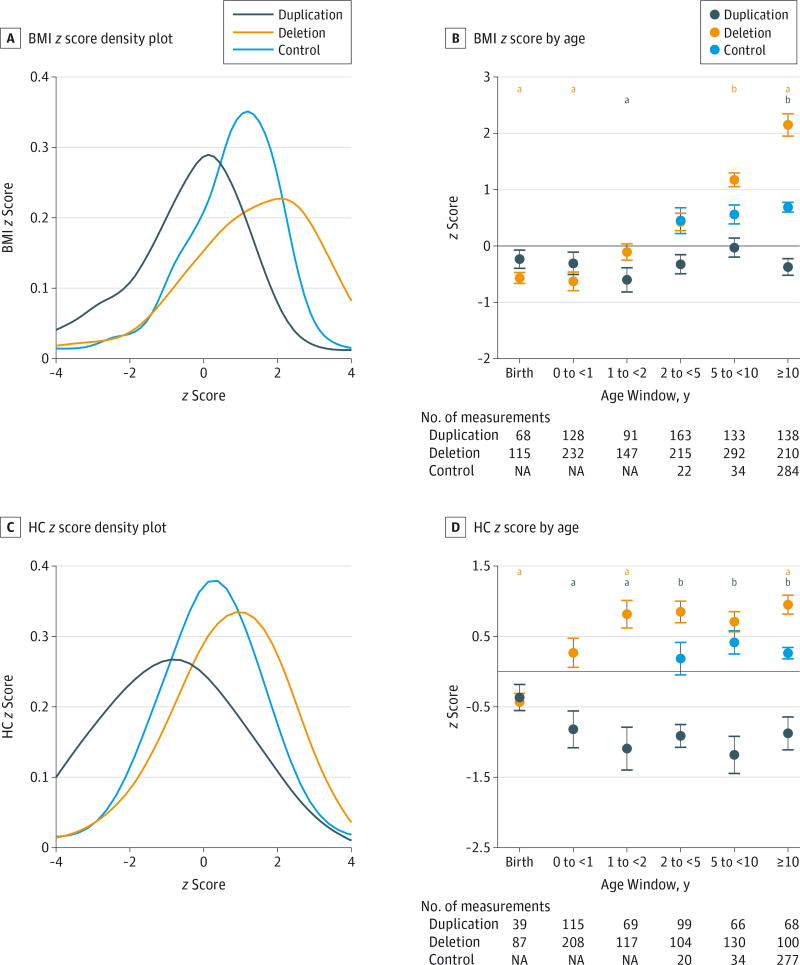
Results: Among the 1006 study participants, the duplication was associated with a mean FSIQ score that was lower by 26.3 points between proband carriers and noncarrier relatives and a lower mean FSIQ score (16.2-11.4 points) in nonproband carriers. The mean overall effect of the deletion was similar (-22.1 points; P < .001). However, broad variation in FSIQ was found, with a 19.4- and 2.0-fold increase in the proportion of FSIQ scores that were very low (≤40) and higher than the mean (>100) compared with the deletion group (P < .001). Parental FSIQ predicted part of this variation (approximately 36.0% in hereditary probands). Although the frequency of ASD was similar in deletion and duplication proband carriers (16.0% and 20.0%, respectively), the FSIQ was significantly lower (by 26.3 points) in the duplication probands with ASD. There also were lower head circumference and BMI measurements among duplication carriers, which is consistent with the findings of previous studies.
Conclusions and relevance: The mean effect of the duplication on cognition is similar to that of the reciprocal deletion, but the variance in the duplication is significantly higher, with severe and mild subgroups not observed with the deletion. These results suggest that additional genetic and familial factors contribute to this variability. Additional studies will be necessary to characterize the predictors of cognitive deficits.
Conflict of interest statement
Figures
Comment in
-
Following the Trail From Genotype to Phenotypes.JAMA Psychiatry. 2016 Jan;73(1):7-8. doi: 10.1001/jamapsychiatry.2015.2344. JAMA Psychiatry. 2016. PMID: 26630619 No abstract available.
References
-
- Weiss LA, Shen Y, Korn JM, et al. Autism Consortium. Association between microdeletion and microduplication at 16p11.2 and autism. N Engl J Med. 2008;358(7):667–675. - PubMed
-
- Kumar RA, Kara Mohamed S, Sudi J, et al. Recurrent 16p11.2microdeletions in autism. Hum Mol Genet. 2008;17(4):628–638. - PubMed
