

Pulmonary Hypertension in Patients with Chronic Fibrosing Idiopathic Interstitial Pneumonias
- PMID: 26630396
- PMCID: PMC4667900
- DOI: 10.1371/journal.pone.0141911
Pulmonary Hypertension in Patients with Chronic Fibrosing Idiopathic Interstitial Pneumonias
Abstract
Background: Pulmonary hypertension (PH) is a common finding in patients with chronic fibrosing idiopathic interstitial pneumonias (IIP). Little is known about the response to pulmonary vasodilator therapy in this patient population. COMPERA is an international registry that prospectively captures data from patients with various forms of PH receiving pulmonary vasodilator therapies.
Methods: We retrieved data from COMPERA to compare patient characteristics, treatment patterns, response to therapy and survival in newly diagnosed patients with idiopathic pulmonary arterial hypertension (IPAH) and PH associated with IIP (PH-IIP).
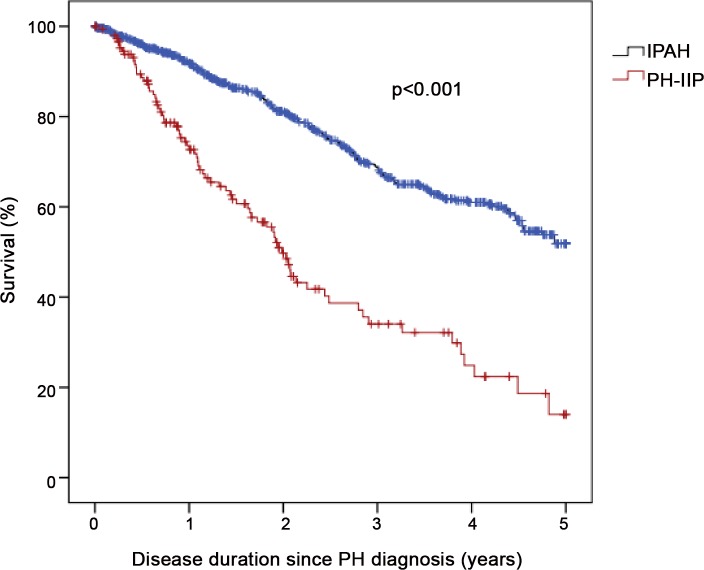
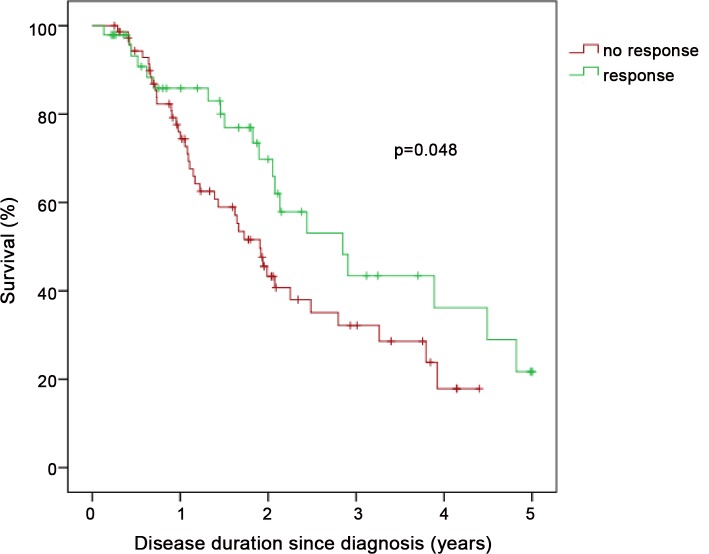
Results: Compared to patients with IPAH (n = 798), patients with PH-IIP (n = 151) were older and predominantly males. Patients with PH-IIP were treated predominantly with phosphodiesterase-5 inhibitors (88% at entry, 87% after 1 year). From baseline to the first follow-up visit, the median improvement in 6MWD was 30 m in patients with IPAH and 24.5 m in patients with PH-IIP (p = 0.457 for the difference between both groups). Improvements in NYHA functional class were observed in 22.4% and 29.5% of these patients, respectively (p = 0.179 for the difference between both groups). Survival rates were significantly worse in PH-IIP than in IPAH (3-year survival 34.0 versus 68.6%; p<0.001). Total lung capacity, NYHA class IV, and mixed-venous oxygen saturation were independent predictors of survival in patients with PH-IIP.
Conclusions: Patients with PH-IIP have a dismal prognosis. Our results suggest that pulmonary vasodilator therapy may be associated with short-term functional improvement in some of these patients but it is unclear whether this treatment affects survival.
Trial registration: clinicaltrials.gov NCT01347216.
Conflict of interest statement
Figures
References
-
- Travis WD, Costabel U, Hansell DM, King TE Jr., Lynch DA, Nicholson AG, et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188(6):733–48. 10.1164/rccm.201308-1483ST . - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
