

Relapse risk of endometrial hyperplasia after treatment with the levonorgestrel-impregnated intrauterine system or oral progestogens
- PMID: 26630538
- PMCID: PMC5215722
- DOI: 10.1111/1471-0528.13763
Relapse risk of endometrial hyperplasia after treatment with the levonorgestrel-impregnated intrauterine system or oral progestogens
Abstract
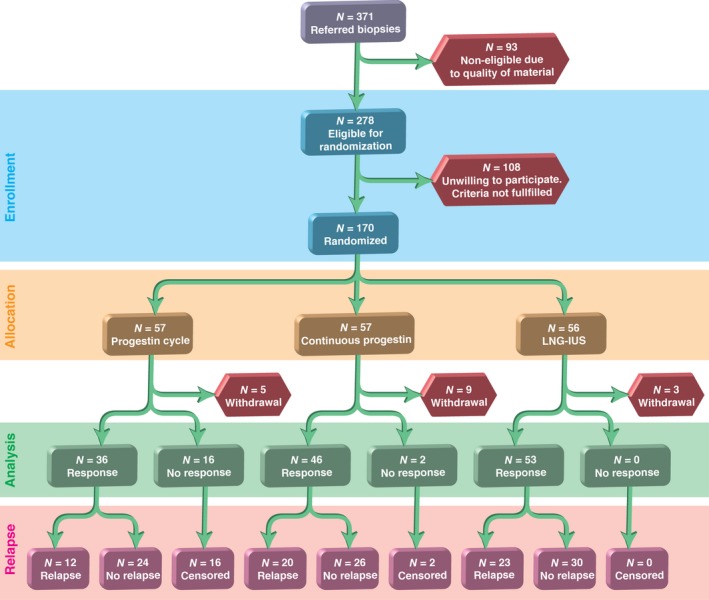
Objective: To investigate relapse rates after the successful treatment of patients with non-atypical endometrial hyperplasia who were randomised to either a levonorgestrel-impregnated intrauterine system (LNG-IUS; Mirena(®) ) or two regimens of oral medroxyprogesterone acetate (MPA) after primary histological response.
Design: A multicentre randomised trial.
Setting: Ten different outpatient clinics localised in hospitals and seven gynaecological private practices in Norway.
Population: One hundred and fifty-three women aged 30-70 years with low- or medium-risk endometrial hyperplasia met the inclusion criteria, and 153 completed the therapy.
Methods: Patients were randomly assigned to one of the following three treatment arms: LNG-IUS; 10 mg of oral MPA administered for 10 days per cycle for 6 months; or 10 mg of oral MPA administered daily for 6 months. The women were followed for 24 months after ending therapy.
Main outcome measures: Histological relapse of endometrial hyperplasia.
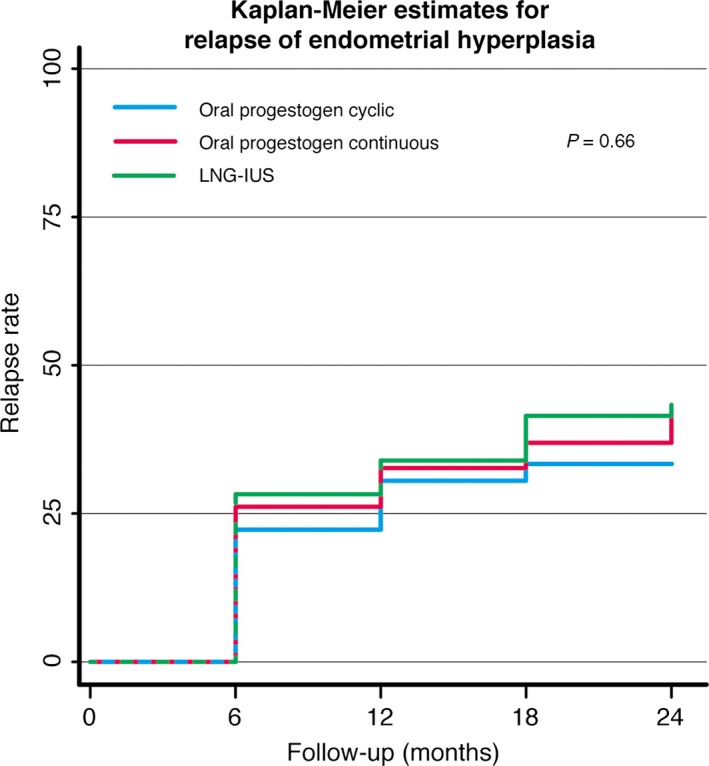
Results: Histological relapse was observed in 55/135 (41%) women who had an initial complete treatment response. The relapse rates were similar in the three therapy groups (P = 0.66). In the multivariable analyses relapse was dependent on menopausal status (P = 0.0005) and estrogen level (P = 0.0007).
Conclusions: The risk of histological relapse of non-atypical endometrial hyperplasia is high within 24 months of ceasing therapy with either the LNG-IUS or oral MPA. Continued endometrial surveillance and prolonging progestogen therapy should be considered.
Tweetable abstract: Relapse of endometrial hyperplasia after successful treatment is independent of therapy regime.
Keywords: Endometrial hyperplasia; levonorgestrel-impregnated intrauterine system; medroxyprogesterone acetate relapse of endometrial hyperplasia; recurrence of endometrial hyperplasia.
© 2015 Royal College of Obstetricians and Gynaecologists.
Figures
Comment in
-
Risk of relapse of endometrial hyperplasia is high and long-term treatment and follow up are recommended.BJOG. 2016 Aug;123(9):1520. doi: 10.1111/1471-0528.13966. Epub 2016 Mar 11. BJOG. 2016. PMID: 26969840 No abstract available.
References
-
- Kurman RJ, Kaminski PF, Norris HJ. The behavior of endometrial hyperplasia. A long‐term study of “untreated” hyperplasia in 170 patients. Cancer 1985;56:403–12. - PubMed
-
- Gallos ID, Shehmar M, Thangaratinam S, Papapostolou TK, Coomarasamy A, Gupta JK. Oral progestogens vs levonorgestrel‐releasing intrauterine system for endometrial hyperplasia: a systematic review and metaanalysis. Am J Obstet Gynecol 2010;203:547.e1–10. - PubMed
-
- Gallos ID, Krishan P, Shehmar M, Ganesan R, Gupta JK. LNG‐IUS versus oral progestogen treatment for endometrial hyperplasia: a long‐term comparative cohort study. Hum Reprod 2013;28:2966–71. - PubMed
-
- Vereide AB, Arnes M, Straume B, Maltau JM, Ørbo A. Nuclear morphometric changes and therapy monitoring in patients with endometrial hyperplasia: a study comparing effects of intrauterine levonorgestrel and systemic medroxyprogesterone. Gynecol Oncol 2003;91:526–33. - PubMed
-
- Ørbo A, Arnes M, Hancke C, Vereide AB, Pettersen I, Larsen K. Treatment results of endometrial hyperplasia after prospective D‐score classification: a follow‐up study comparing effect of LNG‐IUD and oral progestins versus observation only. Gynecol Oncol 2008;111:68–73. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
