

Evaluation of an active magnetic resonance tracking system for interstitial brachytherapy
- PMID: 26632065
- PMCID: PMC4662673
- DOI: 10.1118/1.4935535
Evaluation of an active magnetic resonance tracking system for interstitial brachytherapy
Abstract
Purpose: In gynecologic cancers, magnetic resonance (MR) imaging is the modality of choice for visualizing tumors and their surroundings because of superior soft-tissue contrast. Real-time MR guidance of catheter placement in interstitial brachytherapy facilitates target coverage, and would be further improved by providing intraprocedural estimates of dosimetric coverage. A major obstacle to intraprocedural dosimetry is the time needed for catheter trajectory reconstruction. Herein the authors evaluate an active MR tracking (MRTR) system which provides rapid catheter tip localization and trajectory reconstruction. The authors assess the reliability and spatial accuracy of the MRTR system in comparison to standard catheter digitization using magnetic resonance imaging (MRI) and CT.
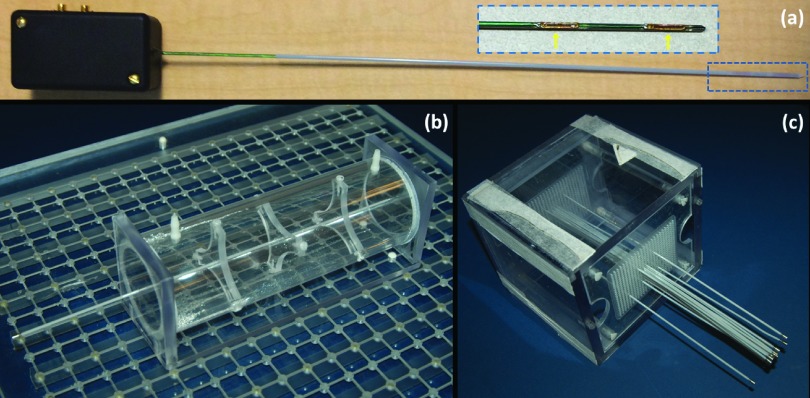
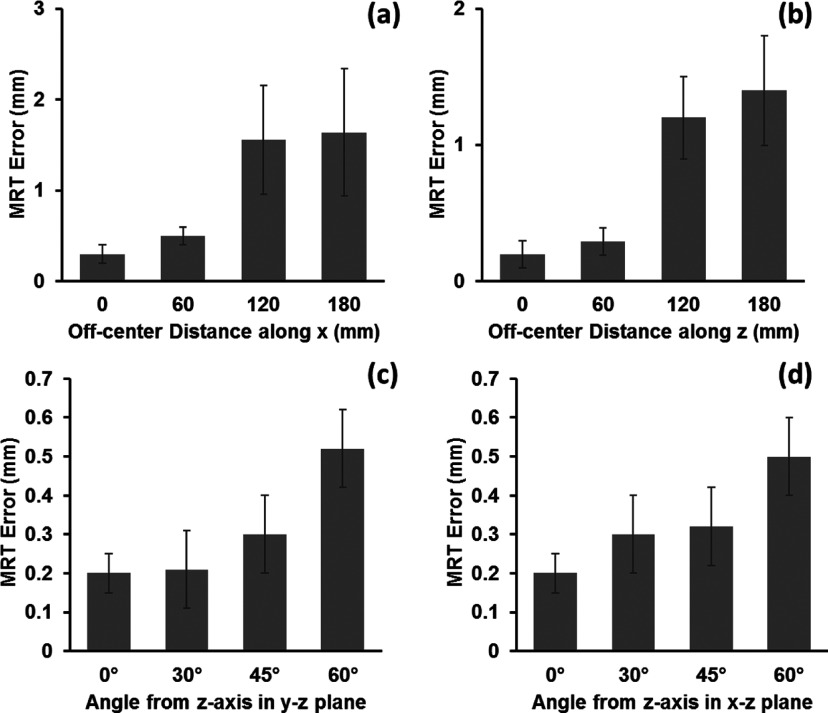
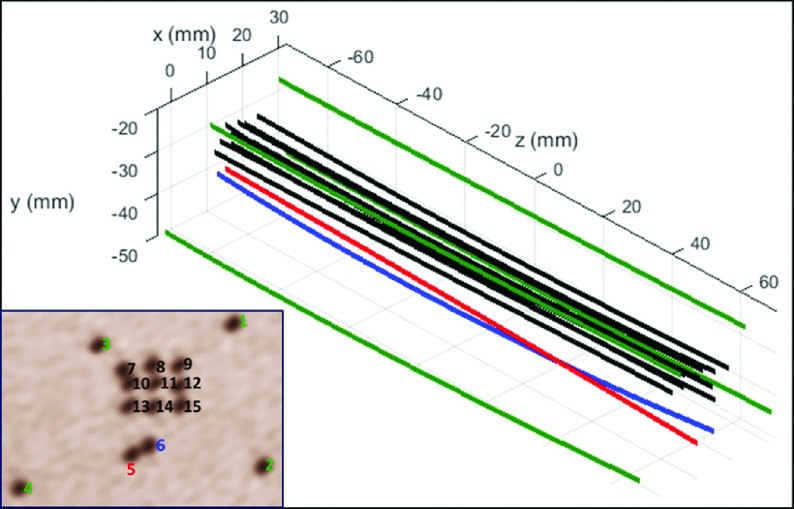
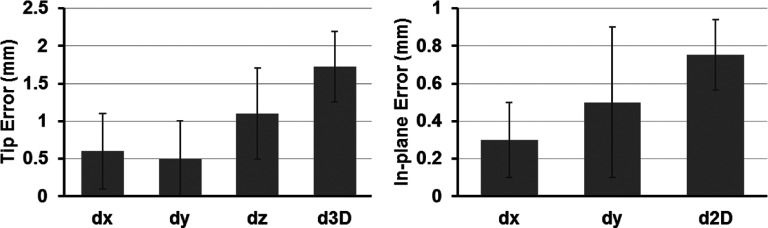
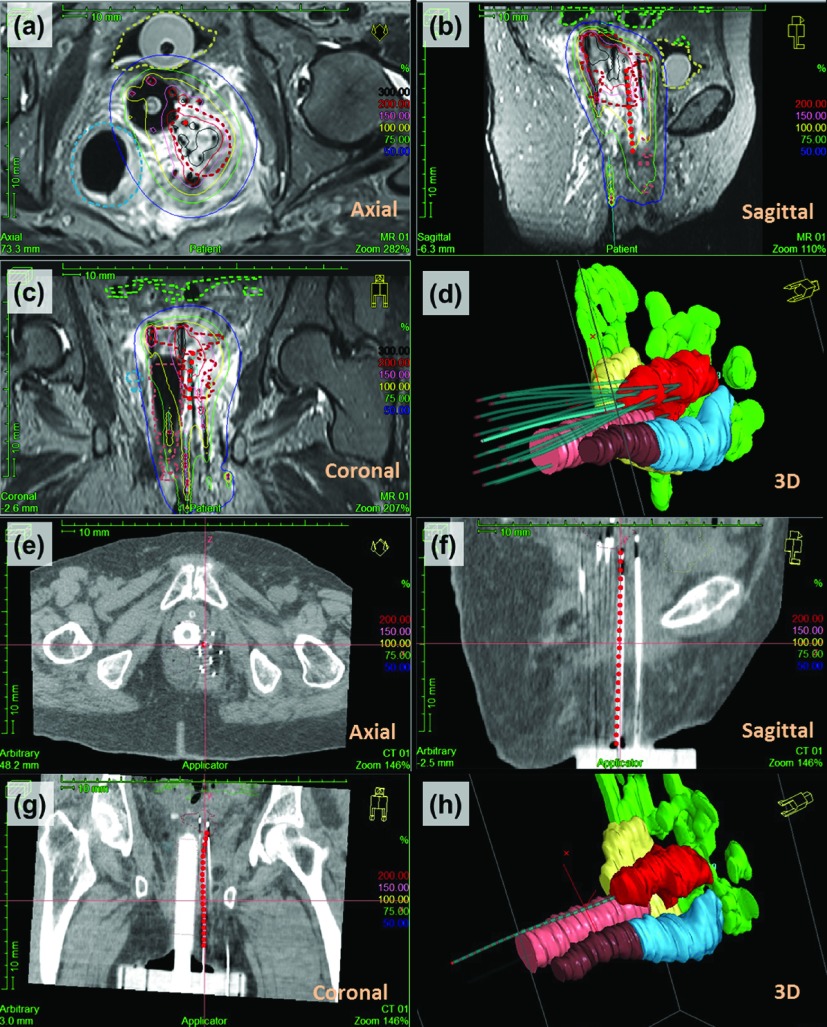
Methods: The MRTR system includes a stylet with microcoils mounted on its shaft, which can be inserted into brachytherapy catheters and tracked by a dedicated MRTR sequence. Catheter tip localization errors of the MRTR system and their dependence on catheter locations and orientation inside the MR scanner were quantified with a water phantom. The distances between the tracked tip positions of the MRTR stylet and the predefined ground-truth tip positions were calculated for measurements performed at seven locations and with nine orientations. To evaluate catheter trajectory reconstruction, fifteen brachytherapy catheters were placed into a gel phantom with an embedded catheter fixation framework, with parallel or crossed paths. The MRTR stylet was then inserted sequentially into each catheter. During the removal of the MRTR stylet from within each catheter, a MRTR measurement was performed at 40 Hz to acquire the instantaneous stylet tip position, resulting in a series of three-dimensional (3D) positions along the catheter's trajectory. A 3D polynomial curve was fit to the tracked positions for each catheter, and equally spaced dwell points were then generated along the curve. High-resolution 3D MRI of the phantom was performed followed by catheter digitization based on the catheter's imaging artifacts. The catheter trajectory error was characterized in terms of the mean distance between corresponding dwell points in MRTR-generated catheter trajectory and MRI-based catheter digitization. The MRTR-based catheter trajectory reconstruction process was also performed on three gynecologic cancer patients, and then compared with catheter digitization based on MRI and CT.
Results: The catheter tip localization error increased as the MRTR stylet moved further off-center and as the stylet's orientation deviated from the main magnetic field direction. Fifteen catheters' trajectories were reconstructed by MRTR. Compared with MRI-based digitization, the mean 3D error of MRTR-generated trajectories was 1.5 ± 0.5 mm with an in-plane error of 0.7 ± 0.2 mm and a tip error of 1.7 ± 0.5 mm. MRTR resolved ambiguity in catheter assignment due to crossed catheter paths, which is a common problem in image-based catheter digitization. In the patient studies, the MRTR-generated catheter trajectory was consistent with digitization based on both MRI and CT.
Conclusions: The MRTR system provides accurate catheter tip localization and trajectory reconstruction in the MR environment. Relative to the image-based methods, it improves the speed, safety, and reliability of the catheter trajectory reconstruction in interstitial brachytherapy. MRTR may enable in-procedural dosimetric evaluation of implant target coverage.
Figures
References
-
- Khan F. M. and Gerbi B. J., Treatment Planning in Radiation Oncology (Lippincott Williams & Wilkins, Philadelphia, PA, 2007).
-
- Polgar C., Major T., Fodor J., Sulyok Z., Somogyi A., Lovey K., Nemeth G., and Kasler M., “Accelerated partial-breast irradiation using high-dose-rate interstitial brachytherapy: 12-year update of a prospective clinical study,” Radiother. Oncol. 94, 274–279 (2010).10.1016/j.radonc.2010.01.019 - DOI - PubMed
-
- Yamada Y., Rogers L., Demanes D. J., Morton G., Prestidge B. R., Pouliot J., Cohen G. N., Zaider M., Ghilezan M., Hsu I. C., and American Brachytherapy Society, “American Brachytherapy Society consensus guidelines for high-dose-rate prostate brachytherapy,” Brachytherapy 11, 20–32 (2012).10.1016/j.brachy.2011.09.008 - DOI - PubMed
-
- Mesko S., Swamy U., Park S. J., Borja L., Wang J., Demanes D. J., and Kamrava M., “Early clinical outcomes of ultrasound-guided CT-planned high-dose-rate interstitial brachytherapy for primary locally advanced cervical cancer,” Brachytherapy 14, 626–632 (2015).10.1016/j.brachy.2015.04.006 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
