

Clinical asthma phenotypes in the real world: opportunities and challenges
- PMID: 26632421
- PMCID: PMC4666449
- DOI: 10.1183/20734735.008115
Clinical asthma phenotypes in the real world: opportunities and challenges
Abstract
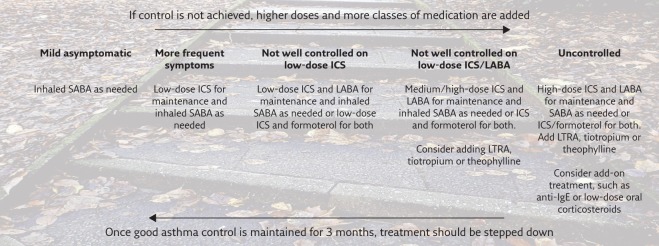
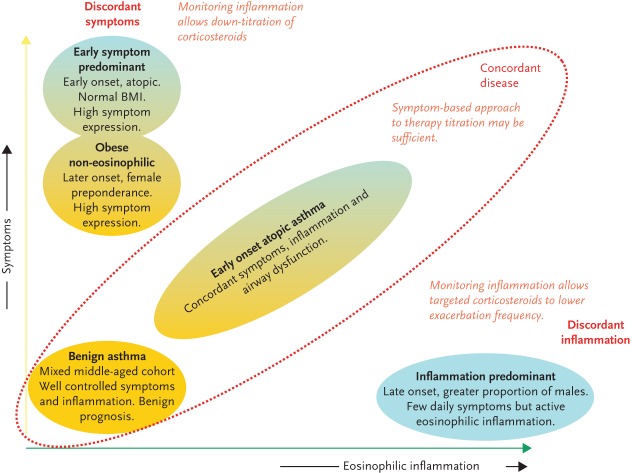
Asthma is a common, chronic and heterogeneous syndrome, affecting people of all ages, all races and both sexes. It may range from mild disease with barely noticeable symptoms, to very severe disease with constant symptoms that greatly hinder the life of the patient. Guidelines issued by various medical societies provide guidance on how to diagnose and manage asthmatic patients. It is now increasingly recognised that asthma management must be individualised, tailored not only to the severity of the disease but to the phenotypic characteristics of each patient. The aim of asthma treatment is control of asthma and the prevention of risk of exacerbations and fixed airflow limitation. Asthma control can be easily assessed clinically through simple screening tools such as the use of validated questionnaires and spirometry. The use of inflammatory biomarkers can be an alternative approach that, however, requires more time and resources. Asthma treatment involves the use of controllers, mainly inhaled corticosteroids and long-acting β2-agonists, and relievers, mainly rapid-acting β2-agonists. Controller medications reduce airway inflammation, lead to better symptom control and reduce the risk of future exacerbations. Reliever (rescue) medications alleviate symptoms and prevent exercise-induced bronchoconstriction. Treatment must be based on a "stepwise approach" in order to achieve good control of symptoms and to minimise future risks of exacerbations. That is, less treatment for mild disease, more treatment for severe, uncontrolled disease. Once good asthma control has been achieved and maintained, treatment should be stepped down. In severe asthmatics, phenotypic characterisation becomes more clinically useful and add-on treatment such as anti-immunoglobulin E monoclonal antibodies may be required. Despite our better understanding of asthma, there are still patients who will not respond to treatment and remain symptomatic. Dissemination of guidelines and national plans allowing early diagnosis of asthma as well as access to specialised primary and secondary care for asthmatic patients, personalised treatment and continuity of care may lead to excellence in care and controlled asthma for the majority of patients. Education of the patient in asthma is also very important, as in every chronic disease, as the patients live with the disease every day while they visit a healthcare professional a few times a year. Future planning for new treatments should focus on the needs of such severe asthma patients.
Conflict of interest statement
Conflict of interestNone declared.
Figures
Similar articles
-
Expert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of Asthma-Summary Report 2007.J Allergy Clin Immunol. 2007 Nov;120(5 Suppl):S94-138. doi: 10.1016/j.jaci.2007.09.043. J Allergy Clin Immunol. 2007. PMID: 17983880
-
Medical Therapy for Asthma: Updates from the NAEPP Guidelines.Am Fam Physician. 2010 Nov 15;82(10):1242-51. Am Fam Physician. 2010. PMID: 21121536 Review.
-
Second-line controller therapy for persistent asthma uncontrolled on inhaled corticosteroids: the step 3 dilemma.Drugs. 2002;62(16):2315-32. doi: 10.2165/00003495-200262160-00001. Drugs. 2002. PMID: 12396225 Review.
-
Nocturnal asthma uncontrolled by inhaled corticosteroids: theophylline or long-acting beta2 agonists?Drugs. 2001;61(3):391-418. doi: 10.2165/00003495-200161030-00007. Drugs. 2001. PMID: 11293649 Review.
-
It is time to change the way we manage mild asthma: an update in GINA 2019.Respir Res. 2019 Aug 14;20(1):183. doi: 10.1186/s12931-019-1159-y. Respir Res. 2019. PMID: 31412856 Free PMC article.
Cited by
-
Cellular Na+ handling mechanisms involved in airway smooth muscle contraction (Review).Int J Mol Med. 2017 Jul;40(1):3-9. doi: 10.3892/ijmm.2017.2993. Epub 2017 May 17. Int J Mol Med. 2017. PMID: 28534960 Free PMC article. Review.
-
Innovations in asthma therapy: is there a role for inhaled statins?Expert Rev Respir Med. 2018 Jun;12(6):461-473. doi: 10.1080/17476348.2018.1457437. Epub 2018 May 3. Expert Rev Respir Med. 2018. PMID: 29575963 Free PMC article. Review.
-
The diagnosis of asthma. Can physiological tests of small airways function help?Chron Respir Dis. 2021 Jan-Dec;18:14799731211053332. doi: 10.1177/14799731211053332. Chron Respir Dis. 2021. PMID: 34693751 Free PMC article. Review.
-
MDSCs Aggravate the Asthmatic Progression in Children and OVA-Allergic Mice by Regulating the Th1/Th2/Th17 Responses.Evid Based Complement Alternat Med. 2022 Aug 22;2022:6157385. doi: 10.1155/2022/6157385. eCollection 2022. Evid Based Complement Alternat Med. 2022. PMID: 36045657 Free PMC article.
-
Effect of outdoor air pollution on asthma exacerbations in children and adults: Systematic review and multilevel meta-analysis.PLoS One. 2017 Mar 20;12(3):e0174050. doi: 10.1371/journal.pone.0174050. eCollection 2017. PLoS One. 2017. PMID: 28319180 Free PMC article.
References
-
- From the Global Strategy for Asthma Management and Prevention, Global Initiative for Asthma (GINA) 2015. http://www.ginasthma.org/
-
- Expert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of Asthma-Summary Report 2007. J Allergy Clin Immunol 2007; 120: Suppl 1, S94–S138. - PubMed
-
- British guideline on the management of asthma. Thorax 2014; 69: 1–192. - PubMed
-
- Reddel HK, Taylor DR, Bateman ED, et al. . An official American Thoracic Society/European Respiratory Society statement: asthma control and exacerbations: standardizing endpoints for clinical asthma trials and clinical practice. Am J Respir Crit Care Med 2009; 180: 59–99. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources