

Current and future directions in the treatment and prevention of drug-induced liver injury: a systematic review
- PMID: 26633044
- PMCID: PMC5074808
- DOI: 10.1586/17474124.2016.1127756
Current and future directions in the treatment and prevention of drug-induced liver injury: a systematic review
Abstract
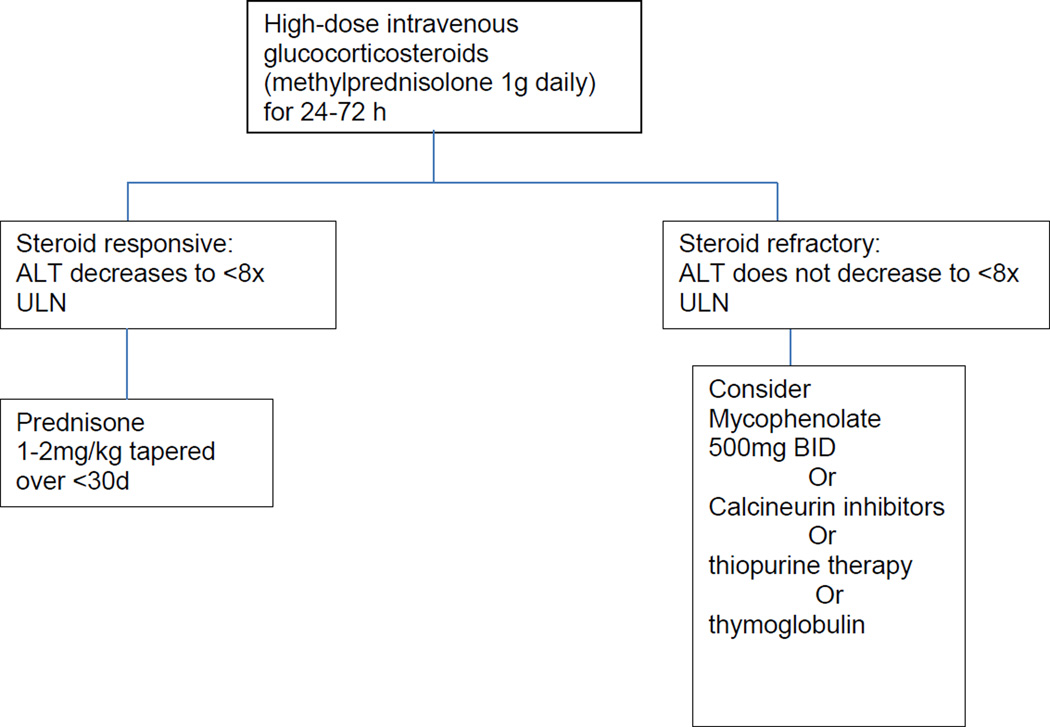
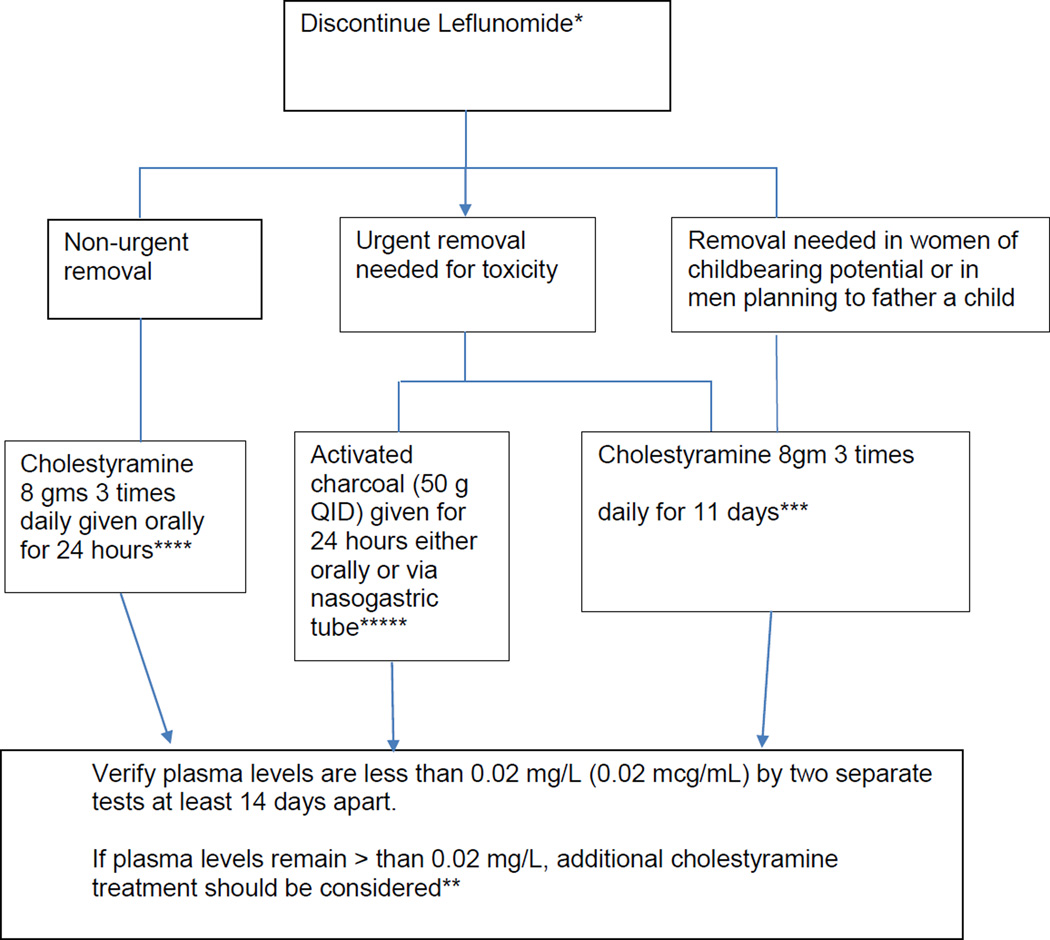
While the pace of discovery of new agents, mechanisms and risk factors involved in drug-induced liver injury (DILI) remains brisk, advances in the treatment of acute DILI seems slow by comparison. In general, the key to treating suspected DILI is to stop using the drug prior to developing irreversible liver failure. However, predicting when to stop is an inexact science, and commonly used ALT monitoring is an ineffective strategy outside of clinical trials. The only specific antidote for acute DILI remains N-acetylcysteine (NAC) for acetaminophen poisoning, although NAC is proving to be beneficial in some cases of non-acetaminophen DILI in adults. Corticosteroids can be effective for DILI associated with autoimmune or systemic hypersensitivity features. Ursodeoxycholic acid, silymarin and glycyrrhizin have been used to treat DILI for decades, but success remains anecdotal. Bile acid washout regimens using cholestyramine appear to be more evidenced based, in particular for leflunomide toxicity. For drug-induced acute liver failure, the use of liver support systems is still investigational in the United States and emergency liver transplant remains limited by its availability. Primary prevention appears to be the key to avoiding DILI and the need for acute treatment. Pharmacogenomics, including human leukocyte antigen genotyping and the discovery of specific DILI biomarkers offers significant promise for the future. This article describes and summarizes the numerous and diverse treatment and prevention modalities that are currently available to manage DILI.
Keywords: DILI; Hepatotoxicity; prevention; treatment.
Conflict of interest statement
Financial and competing interests disclosure The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Figures
References
-
- Lewis JH. The Art and Science of Diagnosing and Managing Drug-induced Liver Injury in 2015 and Beyond. Clin Gastroenterol Hepatol. 2015 - PubMed
-
- Marino G, Zimmerman HJ, Lewis JH. Management of drug-induced liver disease. Current gastroenterology reports. 2001;3(1):38–48. - PubMed
-
- Lewis JH. Drug-Induced Liver Injury Throughout the Drug Development Life Cycle: Where We Have Been, Where We are Now, and Where We are Headed. Perspectives of a Clinical Hepatologist. Pharm Med. 2013;27:165–191.
-
- Chalasani NP, Hayashi PH, Bonkovsky HL, Navarro VJ, Lee WM, Fontana RJ. ACG Clinical Guideline: the diagnosis and management of idiosyncratic drug-induced liver injury. Am J Gastroenterol. 2014;109(7):950–966. quiz 967. - PubMed
-
- Saliba F, Samuel D. Artificial liver support: a real step forward. Minerva medica. 2015;106(1):35–43. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical