

Corticosteroids for treating sepsis
- PMID: 26633262
- PMCID: PMC6494587
- DOI: 10.1002/14651858.CD002243.pub3
Corticosteroids for treating sepsis
Update in
-
Corticosteroids for treating sepsis in children and adults.Cochrane Database Syst Rev. 2019 Dec 6;12(12):CD002243. doi: 10.1002/14651858.CD002243.pub4. Cochrane Database Syst Rev. 2019. Update in: Cochrane Database Syst Rev. 2025 Jun 5;6:CD002243. doi: 10.1002/14651858.CD002243.pub5. PMID: 31808551 Free PMC article. Updated.
Abstract
Background: Sepsis occurs when an infection is complicated by organ failures as defined by a sequential organ failure assessment (SOFA) score of two or higher. Sepsis may be complicated by impaired corticosteroid metabolism. Giving corticosteroids may benefit patients. The original review was published in 2004 and was updated in 2010 and again in 2015.
Objectives: To examine the effects of corticosteroids on death at one month in patients with sepsis, and to examine whether dose and duration of corticosteroids influence patient response to this treatment.
Search methods: We searched the Central Register of Controlled Trials (CENTRAL; 2014, Issue 10), MEDLINE (October 2014), EMBASE (October 2014), Latin American Caribbean Health Sciences Literature (LILACS; October 2014) and reference lists of articles, and we contacted trial authors. The original searches were performed in August 2003 and in October 2009.
Selection criteria: We included randomized controlled trials of corticosteroids versus placebo or supportive treatment in patients with sepsis.
Data collection and analysis: All review authors agreed on the eligibility of trials. One review author extracted data, which were checked by the other review authors, and by the primary author of the paper when possible. We obtained some missing data from trial authors. We assessed the methodological quality of trials.
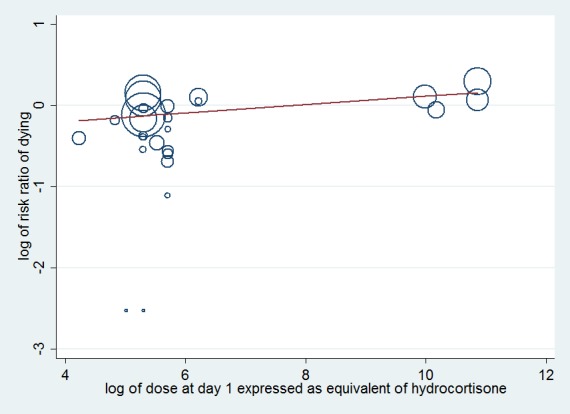
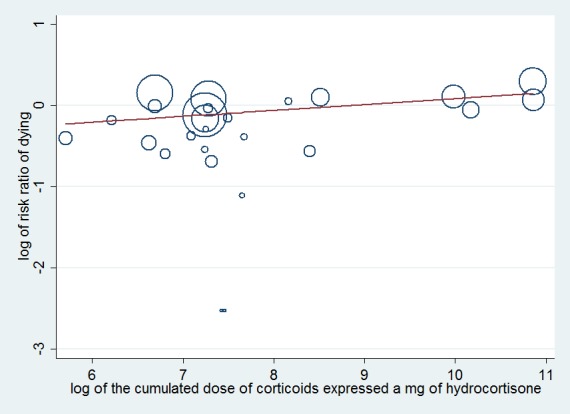
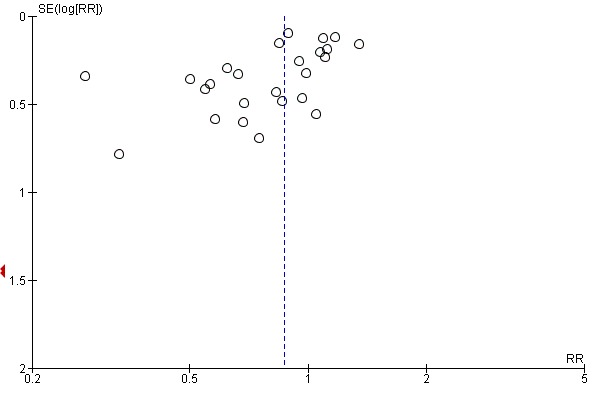
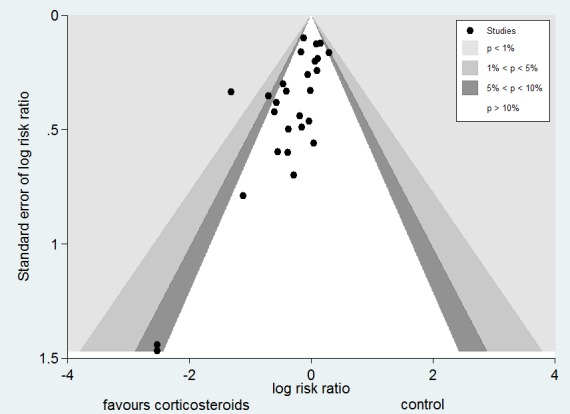
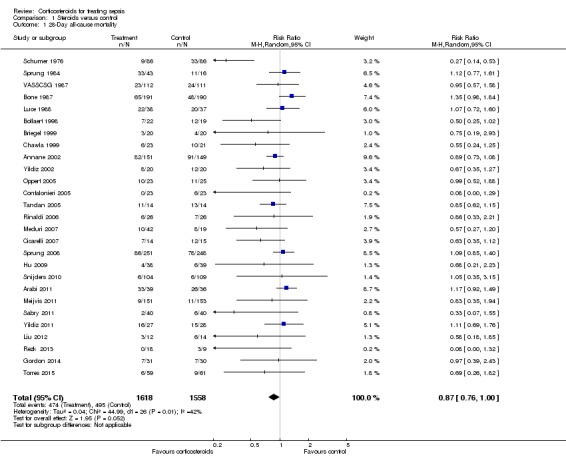
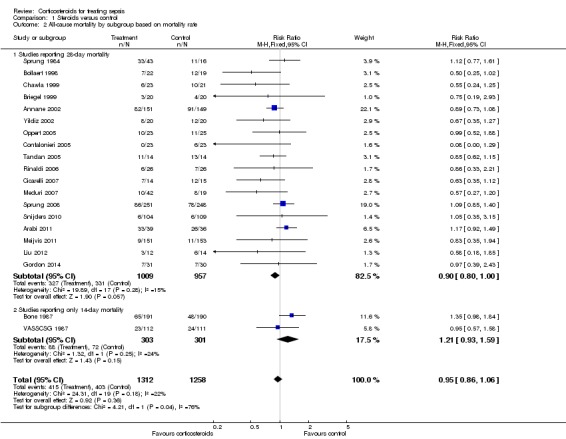
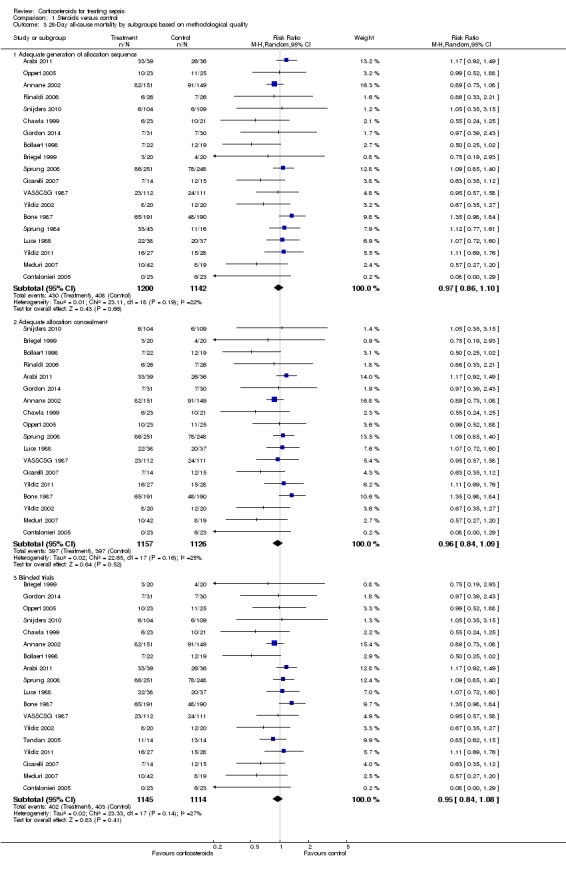
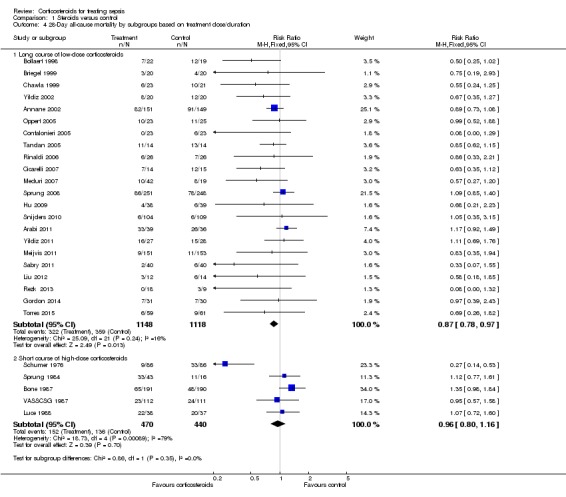
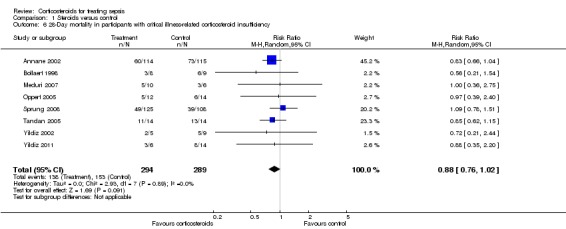
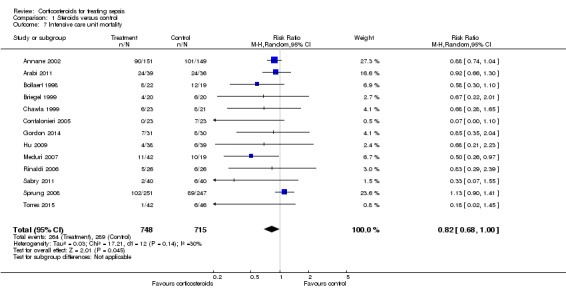
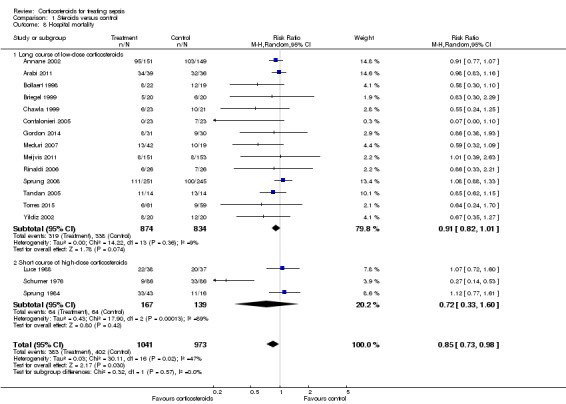
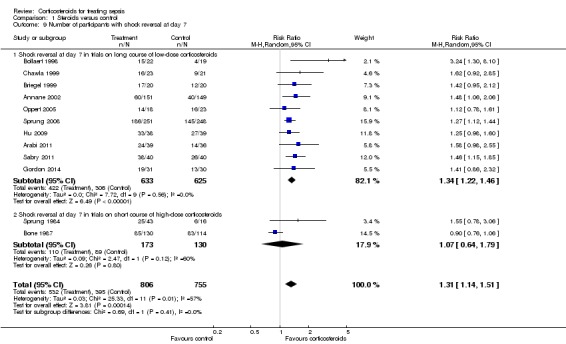
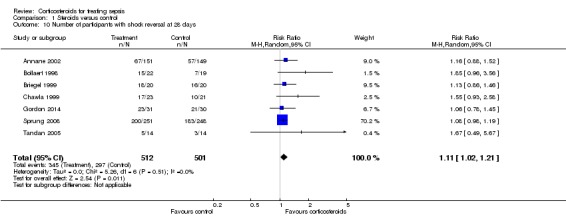
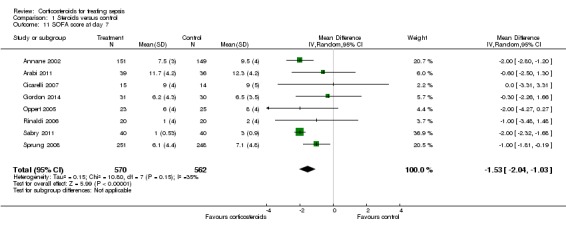
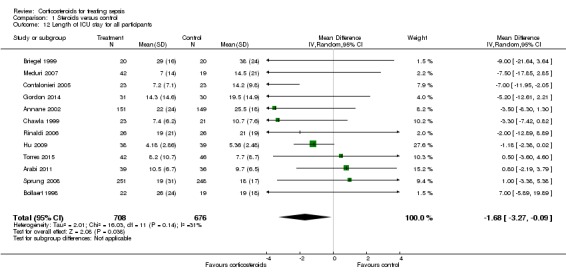
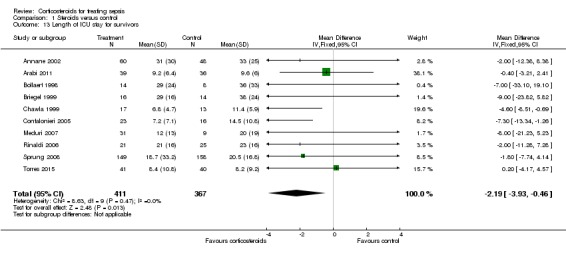
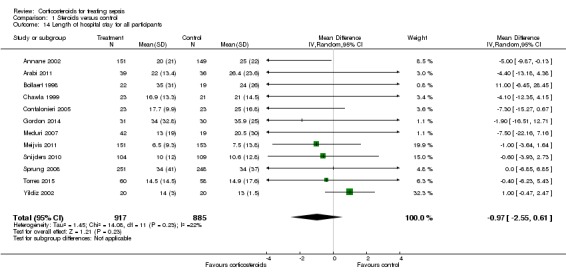
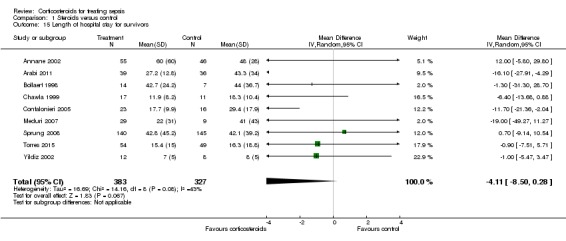
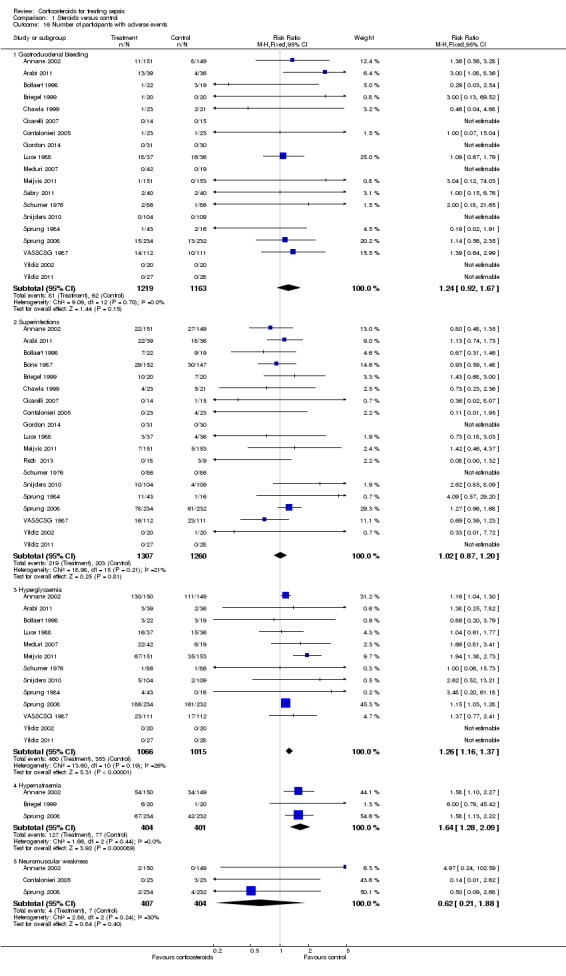
Main results: We identified nine additional studies since the last update, for a total of 33 eligible trials (n = 4268 participants). Twenty-three of these 33 trials were at low risk of selection bias, 22 were at low risk of performance and detection bias, 27 were at low risk of attrition bias and 14 were at low risk of selective reporting.Corticosteroids reduced 28-day mortality (27 trials; n = 3176; risk ratio (RR) 0.87, 95% confidence interval (CI) 0.76 to 1.00; P value = 0.05, random-effects model). The quality of evidence for this outcome was downgraded from high to low for imprecision (upper limit of 95% CI = 1) and for inconsistency (significant heterogeneity across trial results). Heterogeneity was related in part to the dosing strategy. Treatment with a long course of low-dose corticosteroids significantly reduced 28-day mortality (22 trials; RR 0.87, 95% CI 0.78 to 0.97; P value = 0.01, fixed-effect model). The quality of evidence was downgraded from high to moderate for inconsistency (owing to non-significant effects shown by one large trial). Corticosteroids also reduced mortality rate in the intensive care unit (13 trials; RR 0.82, 95% CI 0.68 to 1.00; P value = 0.04, random-effects model) and at the hospital (17 trials; RR 0.85, 95% CI 0.73 to 0.98; P value = 0.03, random-effects model). Quality of the evidence for in-hospital mortality was downgraded from high to moderate for inconsistency and imprecision (upper limit of 95% CI for RR approaching 1). Corticosteroids increased the proportion of shock reversal by day seven (12 trials; RR 1.31, 95% CI 1.14 to 1.51; P value = 0.0001) and by day 28 (seven trials; n = 1013; RR 1.11, 95% CI 1.02 to 1.21; P value = 0.01) and reduced the SOFA score by day seven (eight trials; mean difference (MD) -1.53, 95% CI -2.04 to -1.03; P value < 0.00001, random-effects model) and survivors' length of stay in the intensive care unit (10 trials; MD -2.19, 95% CI -3.93 to -0.46; P value = 0.01, fixed-effect model) without inducing gastroduodenal bleeding (19 trials; RR 1.24, 95% CI 0. 92 to 1.67; P value = 0.15, fixed-effect model), superinfection (19 trials; RR 1.02, 95% CI 0.87 to 1.20; P value = 0.81, fixed-effect model) or neuromuscular weakness (three trials; RR 0.62, 95% CI 0.21 to 1.88; P value = 0.40, fixed-effect model). Corticosteroid increased the risk of hyperglycaemia (13 trials; RR 1.26, 95% CI 1.16 to 1.37; P value < 0.00001, fixed-effect model) and hypernatraemia (three trials; RR 1.64, 95% CI 1.28 to 2.09; P value < 0.0001, fixed-effect model).
Authors' conclusions: Overall, low-quality evidence indicates that corticosteroids reduce mortality among patients with sepsis. Moderate-quality evidence suggests that a long course of low-dose corticosteroids reduced 28-day mortality without inducing major complications and led to an increase in metabolic disorders.
Conflict of interest statement
The following review authors have been involved in randomized controlled trials of low‐dose hydrocortisone that are included in this updated review: Djillali Annane in Annane 2002 and Sprung 2008; Eric Bellissant in Annane 2002; Pierre Edouard Bollaert in Bollaert 1998 and Annane 2002; Josef Briegel in Briegel 1999 and Sprung 2008; Didier Keh in Keh 2003 and Sprung 2008; and Yizhak Kupfer in Chawla 1999.
Djillali Annane is involved with one ongoing study: NCT00625209 2008. This trial is funded by the French Ministry of Social Affairs, Health and Women Rights ‐ Programme Hospitalier de Recherche Clinique PHRC‐12‐002‐0030.
Didier Keh is involved with one ongoing study: NCT00670254 2008. This trial is funded by the Federal Ministry of Education and Research (01KG0701).
Yizhak Kupfer: I am a member of the Pfizer/BMS speakers' bureau for epixaban. This product has no relationship to steroids in sepsis.
Figures



Update of
-
Corticosteroids for treating severe sepsis and septic shock.Cochrane Database Syst Rev. 2004;(1):CD002243. doi: 10.1002/14651858.CD002243.pub2. Cochrane Database Syst Rev. 2004. Update in: Cochrane Database Syst Rev. 2015 Dec 03;(12):CD002243. doi: 10.1002/14651858.CD002243.pub3. PMID: 14973984 Updated.
References
References to studies included in this review
-
- Annane D, Sebille V, Charpentier C, Bollaert PE, François B, Korach JM, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA 2002;288(7):862‐71. [PUBMED: 12186604] - PubMed
-
- COIITSS Study Investigators, Annane D, Cariou A, Maxime V, Azoulay E, D'honneur G, Timsit JF, et al. Corticosteroid treatment and intensive insulin therapy for septic shock in adults: a randomized controlled trial. JAMA 2010;303:341‐8. - PubMed
-
- Bollaert PE, Charpentier C, Levy B, Debouverie M, Audibert G, Larcan A. Reversal of late septic shock with supraphysiologic doses of hydrocortisone. Critical Care Medicine 1998;26(4):645‐50. [PUBMED: 9559600] - PubMed
-
- Bone RG, Fisher CJ, Clemmer TP, Slotman GJ, Metz CA, Balk RA. A controlled clinical trial of high‐dose methylprednisolone in the treatment of severe sepsis and septic shock. New England Journal of Medicine 1987;317(11):653‐8. - PubMed
References to studies excluded from this review
-
- Hughes GS Jr. Naloxone and methylprednisolone sodium succinate enhance sympathomedullary discharge in patients with septic shock. Life Sciences 1984;35(23):2319‐26. [PUBMED: 6390057] - PubMed
-
- Kaufmann I, Briegel J, Schliephake F, Hoelzl A, Chouker A, Hummel T, et al. Stress doses of hydrocortisone in septic shock: beneficial effects on opsonization‐dependent neutrophil functions. Intensive Care Medicine 2008;34:344‐9. [PUBMED: 17906853 ] - PubMed
-
- Klastersky J, Cappel R, Debusscher L. Effectiveness of betamethasone in management of severe infections. A double‐blind study. New England Journal of Medicine 1971;284(22):1248‐50. [PUBMED: 4929896] - PubMed
References to ongoing studies
-
- Blum CA, Nigro N, Briel M, Schuetz P, Ullmer E, Suter‐Widmer I, et al. Adjunct prednisone therapy for patients with community‐acquired pneumonia: a multicentre, double‐blind, randomised, placebo‐controlled trial.. Lancet 2015;385:1511‐8. - PubMed
-
- 6‐Methylprednisolone for multiple organ dysfunction syndrome. Ongoing study 01/08/2005.
-
- Hydrocortisone versus hydrocortisone plus fludrocortisone for treatment of adrenal insufficiency in sepsis. Ongoing studySeptember 2006.
-
- Steroids in patients with early ARDS. Ongoing studyFebruary 2008.
Additional references
-
- ACCP/SCCM Consensus Conference Panel. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Critical Care Medicine 1992;20(6):864‐74. [PUBMED: 1597042 ] - PubMed
-
- Angus DC, Poll T. Severe sepsis and septic shock. New England Journal of Medicine 2013;369:840‐51. - PubMed
-
- Annane D, Sébille V, Troché G, Raphael JC, Gajdos P, Bellissant E. A 3‐level prognostic classification in septic shock based on cortisol levels and cortisol response to corticotropin. JAMA 2000;283(8):1038‐45. [PUBMED: 10697064] - PubMed
-
- Annane D, Aegerter P, Jars‐Guincestre MC, Guidet B, CUB‐Rea Network. Current epidemiology of septic shock: the CUB‐Réa Network. American Journal of Respiratory and Critical Care Medicine 2003;168(2):165‐72. [PUBMED: 12851245] - PubMed
-
- Annane D, Bellissant E, Cavaillon JM. Septic shock. Lancet 2005;365:63‐78. [PUBMED: 15639681] - PubMed
References to other published versions of this review
-
- Annane D, Bellissant E, Bollaert PE, Briegel J, Confalonieri M, Gaudio R, et al. Corticosteroids in the treatment of severe sepsis and septic shock in adults: a systematic review. JAMA 2009;301:2362‐75. [PUBMED: 19509383 ] - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical