

Molecular diagnostic experience of whole-exome sequencing in adult patients
- PMID: 26633545
- PMCID: PMC4892996
- DOI: 10.1038/gim.2015.142
Molecular diagnostic experience of whole-exome sequencing in adult patients
Abstract
Purpose: Whole-exome sequencing (WES) is increasingly used as a diagnostic tool in medicine, but prior reports focus on predominantly pediatric cohorts with neurologic or developmental disorders. We describe the diagnostic yield and characteristics of WES in adults.
Methods: We performed a retrospective analysis of consecutive WES reports for adults from a diagnostic laboratory. Phenotype composition was determined using Human Phenotype Ontology terms.
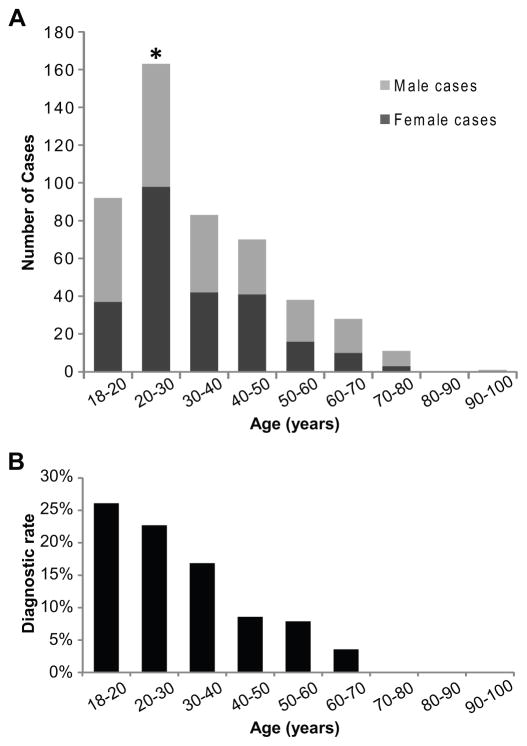
Results: Molecular diagnoses were reported for 17.5% (85/486) of adults, which is lower than that for a primarily pediatric population (25.2%; P = 0.0003); the diagnostic rate was higher (23.9%) for those 18-30 years of age compared to patients older than 30 years (10.4%; P = 0.0001). Dual Mendelian diagnoses contributed to 7% of diagnoses, revealing blended phenotypes. Diagnoses were more frequent among individuals with abnormalities of the nervous system, skeletal system, head/neck, and growth. Diagnostic rate was independent of family history information, and de novo mutations contributed to 61.4% of autosomal dominant diagnoses.
Conclusion: Early WES experience in adults demonstrates molecular diagnoses in a substantial proportion of patients, informing clinical management, recurrence risk, and recommendations for relatives. A positive family history was not predictive, consistent with molecular diagnoses often revealed by de novo events, informing the Mendelian basis of genetic disease in adults.Genet Med 18 7, 678-685.
Conflict of interest statement
Baylor College of Medicine (BCM) and Miraca Holdings Inc. have formed a joint venture with shared ownership and governance of the Baylor Miraca Genetics Laboratories (BMGL), which performs clinical exome sequencing. JAR, ZN, FX, REP, MW, ALB, CME, YY, RAG, JRL, and SEP are employees of BCM and derive support through a professional services agreement with the BMGL. SEP and JRL serve on the Scientific Advisory Board of the BMGL. RAG serves as interim Chief Scientific Officer of the BMGL. ALB serves as Chief Medical Officer of the BMGL.
MB is the founder of Codified Genomics Inc., and derives personal fees from Illumina Inc. SD is the CEO and co-founder of PanGenomics Clinical Genetics Center in India. JAR reports personal fees from Signature Genomic Laboratories, PerkinElmer, Inc., in the past 36 months. RAG reports consulting fees from GE-Clarient. JRL has stock ownership in 23 and Me, is a paid consultant for Regeneron Pharmaceuticals, has stock options in Lasergen, Inc and is a co-inventor on multiple United States and European patents related to molecular diagnostics for inherited neuropathies, eye diseases and bacterial genomic fingerprinting. Other authors have no disclosures relevant to the manuscript.
Other authors have no potential conflicts to disclose.
Figures

Comment in
-
Parental DNA sequence is critical family history in clinical genomics.Genet Med. 2016 Jul;18(7):675-7. doi: 10.1038/gim.2015.177. Epub 2016 Jan 14. Genet Med. 2016. PMID: 26765341 No abstract available.
References
-
- Wheeler DA, Srinivasan M, Egholm M, et al. The complete genome of an individual by massively parallel DNA sequencing. Nature. 2008;452(7189):872–876. - PubMed
-
- Albert TJ, Molla MN, Muzny DM, et al. Direct selection of human genomic loci by microarray hybridization. Nat Methods. 2007;4(11):903–905. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
