

Sustainable HIV treatment in Africa through viral-load-informed differentiated care
- PMID: 26633768
- PMCID: PMC4932825
- DOI: 10.1038/nature16046
Sustainable HIV treatment in Africa through viral-load-informed differentiated care
Abstract
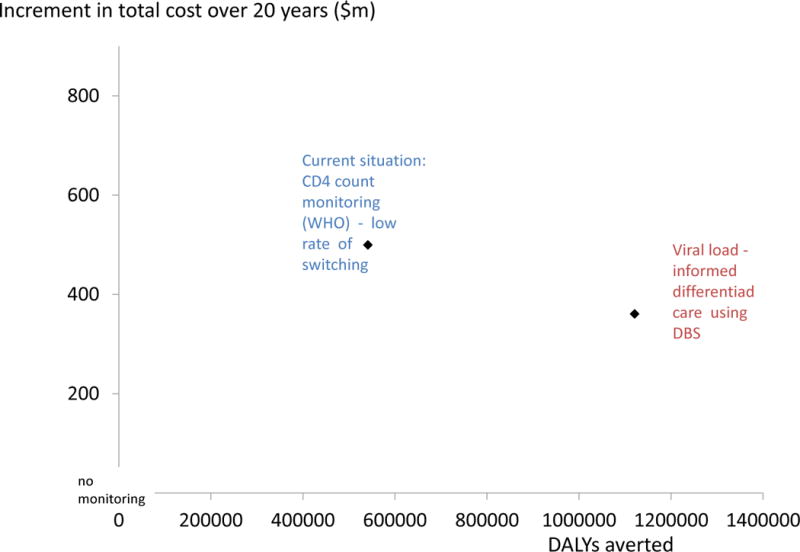
There are inefficiencies in current approaches to monitoring patients on antiretroviral therapy in sub-Saharan Africa. Patients typically attend clinics every 1 to 3 months for clinical assessment. The clinic costs are comparable with the costs of the drugs themselves and CD4 counts are measured every 6 months, but patients are rarely switched to second-line therapies. To ensure sustainability of treatment programmes, a transition to more cost-effective delivery of antiretroviral therapy is needed. In contrast to the CD4 count, measurement of the level of HIV RNA in plasma (the viral load) provides a direct measure of the current treatment effect. Viral-load-informed differentiated care is a means of tailoring care so that those with suppressed viral load visit the clinic less frequently and attention is focussed on those with unsuppressed viral load to promote adherence and timely switching to a second-line regimen. The most feasible approach to measuring viral load in many countries is to collect dried blood spot samples for testing in regional laboratories; however, there have been concerns over the sensitivity and specificity of this approach to define treatment failure and the delay in returning results to the clinic. We use modelling to synthesize evidence and evaluate the cost-effectiveness of viral-load-informed differentiated care, accounting for limitations of dried blood sample testing. We find that viral-load-informed differentiated care using dried blood sample testing is cost-effective and is a recommended strategy for patient monitoring, although further empirical evidence as the approach is rolled out would be of value. We also explore the potential benefits of point-of-care viral load tests that may become available in the future.
Figures







References
-
- Siapka M, Remme M, Dayo Obure C, Maier C, Dehne KL, Vassall A. Is there scope for cost savings and efficiency gains in HIV services? A systematic review of the evidence from low- and middle-income countries. Bull World Health Organ. 2014;92:499–511AD. doi: http://dx.doi.org/10.2471/BLT.13.127639. - DOI - PMC - PubMed
-
- Tagar E, Sundaram M, Condliffe K, Matatiyo B, Chimbwandira F, et al. Multi-Country Analysis of Treatment Costs for HIV/AIDS (MATCH): Facility-Level ART Unit Cost Analysis in Ethiopia, Malawi, Rwanda, South Africa and Zambia. PLoS ONE. 2014;9(11):e108304. doi: 10.1371/journal.pone.0108304. - DOI - PMC - PubMed
-
- World Health Organisation. Technical and operational considerations for implementing HIV viral load testing. Access to HIV diagnostics. 2014 Jul; www.who.int.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
