

Genetic lineage tracing identifies in situ Kit-expressing cardiomyocytes
- PMID: 26634606
- PMCID: PMC4816131
- DOI: 10.1038/cr.2015.143
Genetic lineage tracing identifies in situ Kit-expressing cardiomyocytes
Abstract
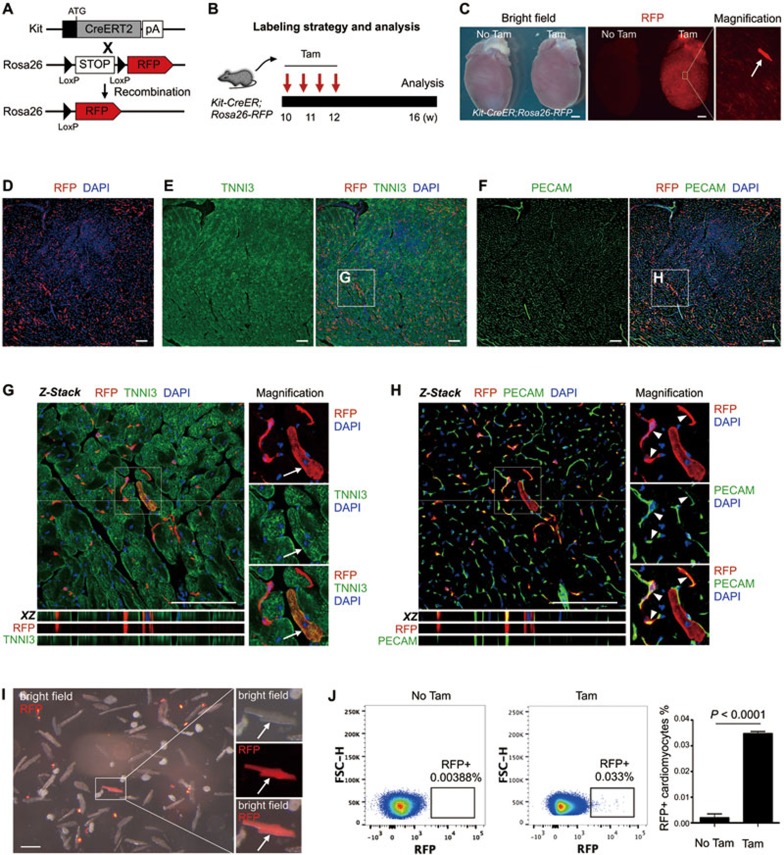
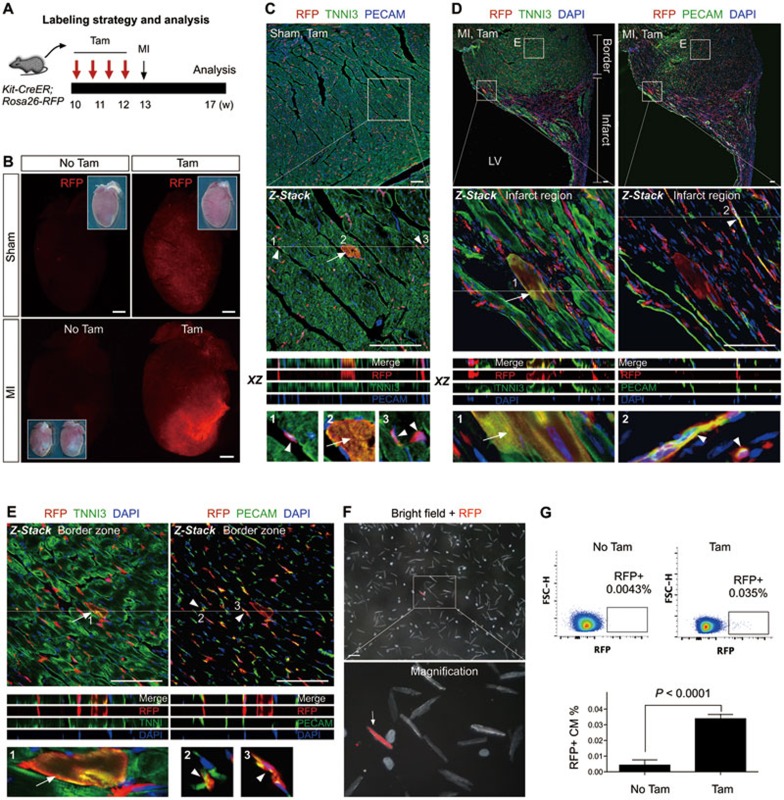
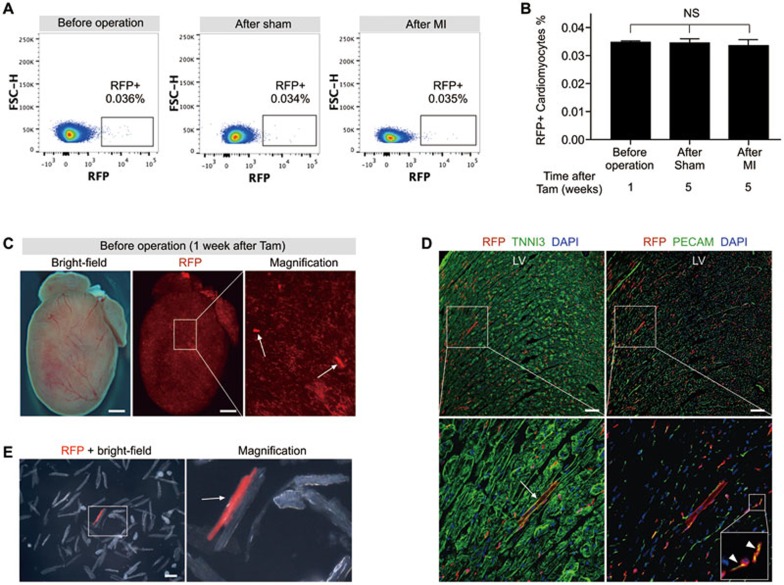
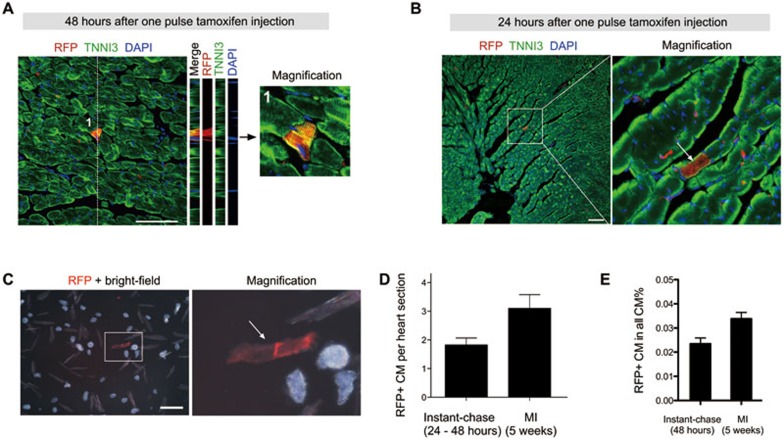
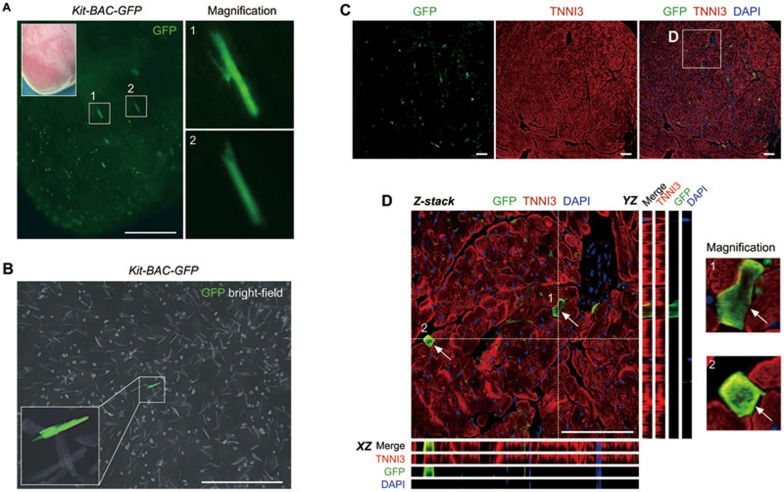
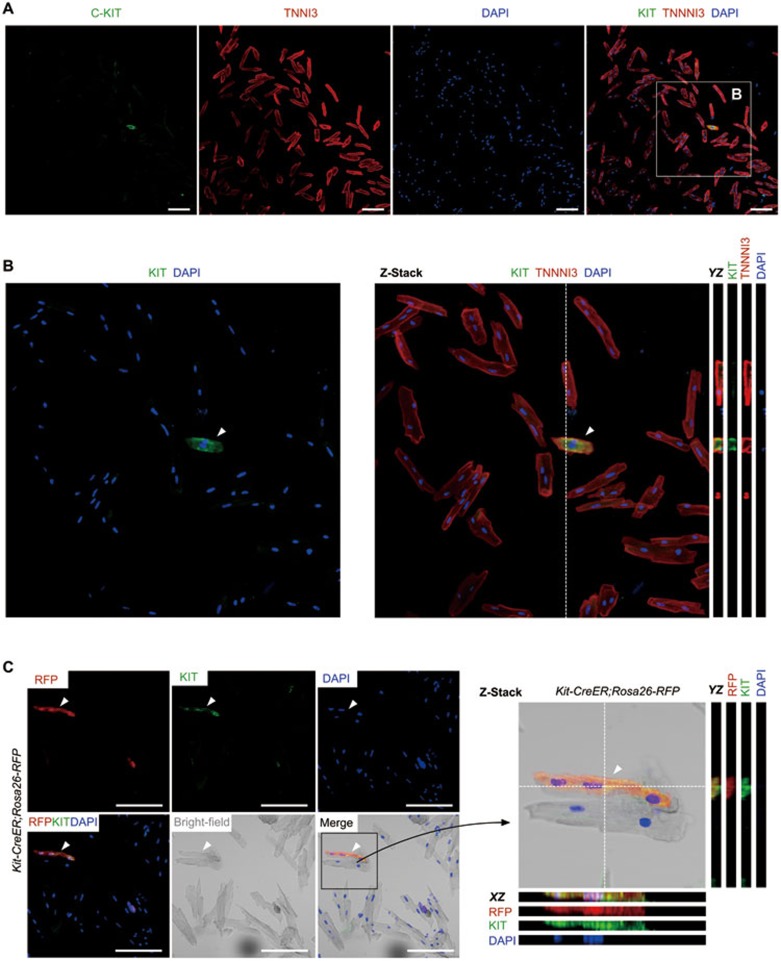
Cardiac cells marked by c-Kit or Kit, dubbed cardiac stem cells (CSCs), are in clinical trials to investigate their ability to stimulate cardiac regeneration and repair. These studies were initially motivated by the purported cardiogenic activity of these cells. Recent lineage tracing studies using Kit promoter to drive expression of the inducible Cre recombinase showed that these CSCs had highly limited cardiogenic activity, inadequate to support efficient cardiac repair. Here we reassess the lineage tracing data by investigating the identity of cells immediately after Cre labeling. Our instant lineage tracing approach identifies Kit-expressing cardiomyocytes, which are labeled immediately after tamoxifen induction. In combination with long-term lineage tracing experiments, these data reveal that the large majority of long-term labeled cardiomyocytes are pre-existing Kit-expressing cardiomyocytes rather than cardiomyocytes formed de novo from CSCs. This study presents a new interpretation for the contribution of Kit(+) cells to cardiomyocytes and shows that Kit genetic lineage tracing over-estimates the cardiogenic activity of Kit(+) CSCs.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
