

Extracorporeal Cardiopulmonary Resuscitation (E-CPR) During Pediatric In-Hospital Cardiopulmonary Arrest Is Associated With Improved Survival to Discharge: A Report from the American Heart Association's Get With The Guidelines-Resuscitation (GWTG-R) Registry
- PMID: 26635402
- PMCID: PMC4814337
- DOI: 10.1161/CIRCULATIONAHA.115.016082
Extracorporeal Cardiopulmonary Resuscitation (E-CPR) During Pediatric In-Hospital Cardiopulmonary Arrest Is Associated With Improved Survival to Discharge: A Report from the American Heart Association's Get With The Guidelines-Resuscitation (GWTG-R) Registry
Abstract
Background: Although extracorporeal cardiopulmonary resuscitation (E-CPR) can result in survival after failed conventional CPR (C-CPR), no large, systematic comparison of pediatric E-CPR and continued C-CPR has been reported.
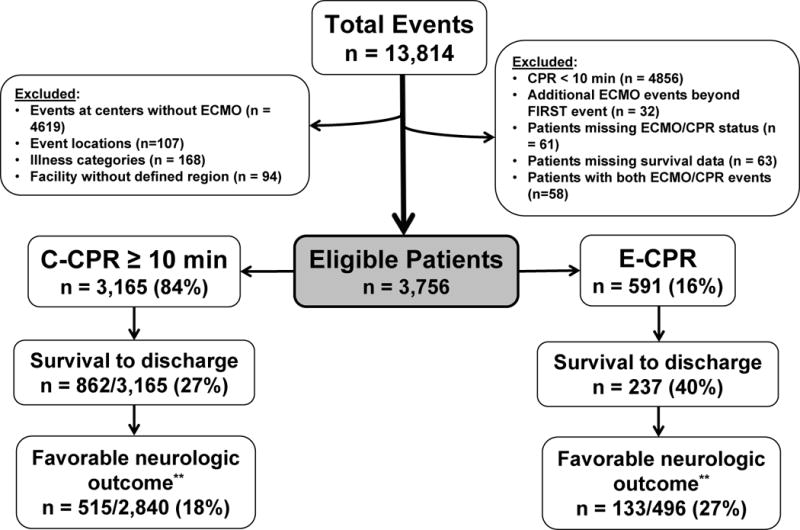
Methods and results: Consecutive patients <18 years old with CPR events ≥10 minutes in duration reported to the Get With the Guidelines-Resuscitation registry between January 2000 and December 2011 were identified. Hospitals were grouped by teaching status and location. Primary outcome was survival to discharge. Regression modeling was performed, conditioning on hospital groups. A secondary analysis was performed with the use of propensity score matching. Of 3756 evaluable patients, 591 (16%) received E-CPR and 3165 (84%) received C-CPR only. Survival to hospital discharge and survival with favorable neurological outcome (Pediatric Cerebral Performance Category score of 1-3 or unchanged from admission) were greater for E-CPR (40% [237 of 591] and 27% [133 of 496]) versus C-CPR patients (27% [862 of 3165] and 18% [512 of 2840]). Odds ratios (ORs) for survival to hospital discharge and survival with favorable neurological outcome were greater for E-CPR versus C-CPR. After adjustment for covariates, patients receiving E-CPR had higher odds of survival to discharge (OR, 2.80; 95% confidence interval, 2.13-3.69; P<0.001) and survival with favorable neurological outcome (OR, 2.64; 95% confidence interval, 1.91-3.64; P<0.001) than patients who received C-CPR. This association persisted when analyzed by propensity score-matched cohorts (OR, 1.70; 95% confidence interval, 1.33-2.18; P<0.001; and OR, 1.78; 95% confidence interval, 1.31-2.41; P<0.001, respectively].
Conclusion: For children with in-hospital CPR of ≥10 minutes duration, E-CPR was associated with improved survival to hospital discharge and survival with favorable neurological outcome compared with C-CPR.
Keywords: cardiopulmonary resuscitation; extracorporeal circulation; heart arrest; mortality; pediatrics.
© 2015 American Heart Association, Inc.
Figures
Comment in
-
Compared to conventional CPR for in-hospital cardiac arrest, extracorporeal-CPR is associated with improved survival to hospital discharge and more favourable neurological outcome.Evid Based Med. 2016 Dec;21(6):227-228. doi: 10.1136/ebmed-2016-110467. Epub 2016 Sep 1. Evid Based Med. 2016. PMID: 27586148 No abstract available.
References
-
- Reis AG, Nadkarni VM, Perondi MB, Grisi S, Berg RA. A Prospective Investigation Into the Epidemiology of In-Hospital Pediatric Cardiopulmonary Resuscitation Using the International Utstein Reporting Style. Pediatrics. 2002;109:200–209. - PubMed
-
- Slonim AD, Patel KM, Ruttimann UE, Pollack MM. Cardiopulmonary resuscitation in pediatric intensive care units. Crit Care Med. 1997;25:1951–1955. - PubMed
-
- de Mos N, van Litsenburg RRL, McCrindle B, Bohn DJ, Parshuram CS. Pediatric in-intensive-care-unit cardiac arrest: Incidence, survival, and predictive factors. Crit Care Med. 2006;34:1209–1215. - PubMed
-
- Parra DA, Totapally BR, Zahn E, Jacobs J, Aldousany A, Burke RP, Chang AC. Outcome of cardiopulmonary resuscitation in a pediatric cardiac intensive care unit. Crit Care Med. 2000;28:3296–3300. - PubMed
-
- Rhodes JF, Blaufox AD, Seiden HS, Asnes JD, Gross RP, Rhodes JP, Griepp RB, Rossi AF. Cardiac Arrest in Infants After Congenital Heart Surgery. Circulation. 1999;100(Supplement 2):II–194–II–199. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
