

Operative versus non-operative treatment in complex proximal humeral fractures: a meta-analysis of randomized controlled trials
- PMID: 26636016
- PMCID: PMC4659794
- DOI: 10.1186/s40064-015-1522-5
Operative versus non-operative treatment in complex proximal humeral fractures: a meta-analysis of randomized controlled trials
Abstract
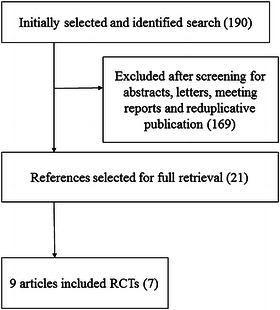
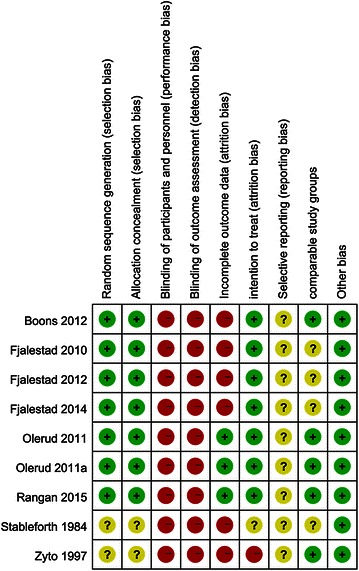
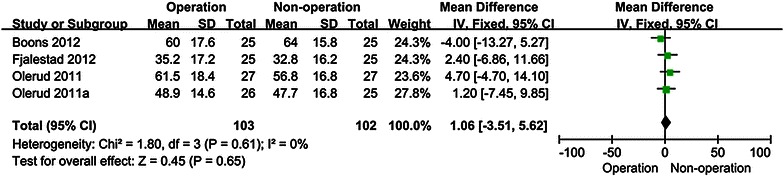
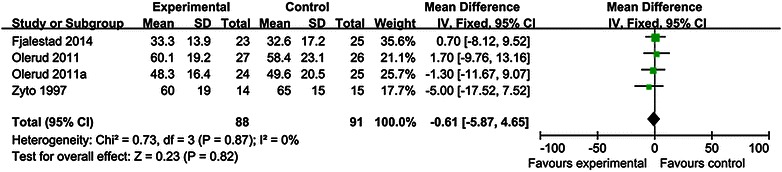
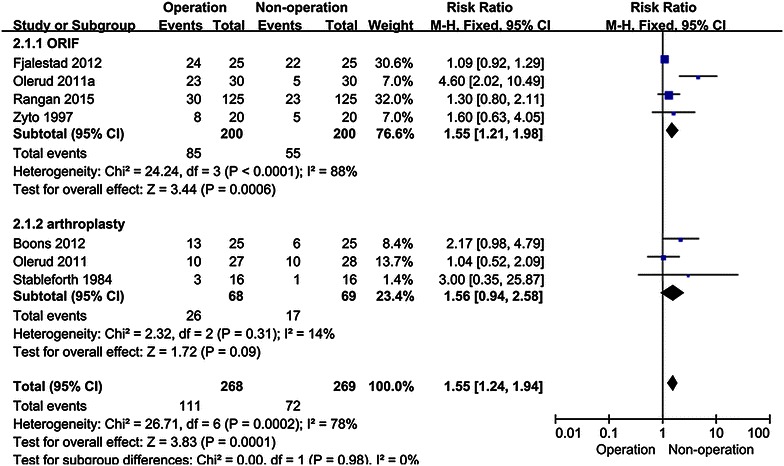
Whether operative treatment for complex proximal humeral fractures (CPHFs) has a greater benefit over non-operative treatment remains controversial. There is no consensus on the optimal treatment in elderly patients with CPHFs. This updated meta-analysis of randomized controlled trials (RCTs) aims to investigate whether operative treatment is superior to non-operative treatment in CPHFs. The authors searched RCTs in the electronic databases (Cochrane Central Register of Controlled Trials, PubMed, EMBASE, Medline, Embase, Springer Link, Web of Knowledge, OVID and Google Scholar) from their establishment to July 2015. Researches on operative and non-operative treatment for CPHFs were selected in this meta-analysis. The quality of all studies was assessed and effective data was pooled for this meta-analysis. Outcome measurements were functional status include constant scores (CS scores) and disabilities of the arm, shoulder and hand scores (DASH scores), total complication rates and healthy-related quality of life. The meta-analysis was performed with software revman 5.3. Nine articles with a total 518 patients (average age 70.93) met inclusion criteria. Patients were followed up for at least 1 year in all the studies. No statistical differences were found between operative and non-operative treatment in CS scores at 12 mo (months) [MD 1.06 95 % CI (-3.51, 5.62)] and 24 mo [MD -0.61 95 % CI (-5.87, 4.65)]. There are also no statistical differences between operative and non-operative treatment in DASH scores at 12 mo [MD -4.51 95 % CI (-13.49, 4.47)] and 24 mo [MD -7.43 95 % CI (-16.14, 1.27)]. Statistical differences were found between operative and non-operative treatment in total complication rates [RR 1.55, 95 % CI (1.24, 1.94)]. Statistical differences in EQ-5D at 24 mo [MD 0.15, 95 % CI (0.05, 0.24)] were found between operative and non-operative treatment but no statistical differences were found in ED-5D at 12 mo [MD 0.08, 95 % CI (-0.01, 0.17)], 15D at 12 mo [MD 0.02, 95 % CI (-0.68, 0.73)] and 15D at 24 mo [MD 0.02, 95 % CI (-0.07, 0.83)]. Operative treatments did not significantly improve the functional outcome and healthy-related quality of life in elderly patients. Instead, Operative treatment for CPHFs led to higher incidence of postoperative complications.
Keywords: Complex proximal humeral fractures (CPHFs); Meta-analysis; Non-operative treatment; Operative; Randomized controlled trials (RCTs).
Figures


References
-
- Baron JA, Karagas M, Barrett J, Kniffin W, Malenka D, Mayor M, Keller RB (1996b) Basic epidemiology of fractures of the upper and lower limb among Americans over 65 years of age. Epidemiology 7(6):612–618. doi:10.1097/00001648-199611000-00008 - PubMed
-
- Bengner U, Johnell O, Redlundjohnell I. Changes in the incidence of fracture of the upper end of the humerus during a 30-year period. A study of 2125 fractures. Clin Orthop Relat R. 1988;231:179–182. - PubMed
-
- Brorson S, Olsen BS, Frich LH, Jensen SL, Johannsen HV, Sorensen AK, Hrobjartsson A. Effect of osteosynthesis, primary hemiarthroplasty, and non-surgical management for displaced four-part fractures of the proximal humerus in elderly: a multi-centre, randomised clinical trial. Trials. 2009;10:51. doi: 10.1186/1745-6215-10-51. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
