

Early Hepatic Dysfunction Is Associated with a Worse Outcome in Patients Presenting with Acute Respiratory Distress Syndrome: A Post-Hoc Analysis of the ACURASYS and PROSEVA Studies
- PMID: 26636318
- PMCID: PMC4670098
- DOI: 10.1371/journal.pone.0144278
Early Hepatic Dysfunction Is Associated with a Worse Outcome in Patients Presenting with Acute Respiratory Distress Syndrome: A Post-Hoc Analysis of the ACURASYS and PROSEVA Studies
Abstract
Introduction: Bilirubin is well-recognized marker of hepatic dysfunction in intensive care unit (ICU) patients. Multiple organ failure often complicates acute respiratory distress syndrome (ARDS) evolution and is associated with high mortality. The effect of early hepatic dysfunction on ARDS mortality has been poorly investigated. We evaluated the incidence and the prognostic significance of increased serum bilirubin levels in the initial phase of ARDS.
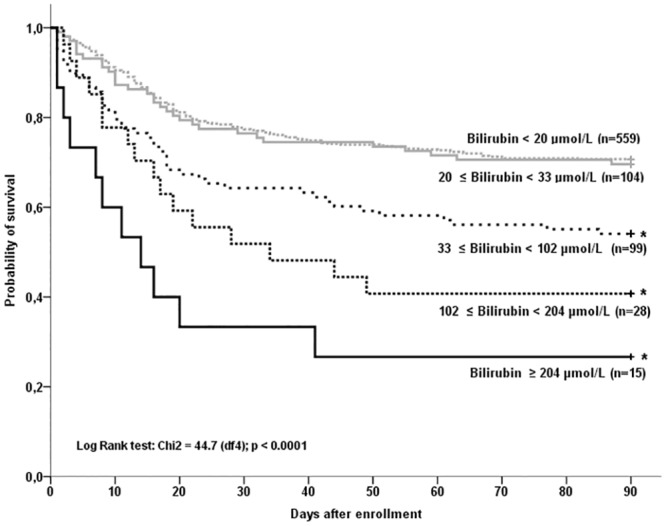
Methods: The data of 805 patients with ARDS were retrospectively analysed. This population was extracted from two recent multicenter, prospective and randomised trials. Patients presenting with ARDS with a ratio of the partial pressure of arterial oxygen to the fraction of inspired oxygen < 150 mmHg measured with a PEEP ≥ 5 cm of water were included. The total serum bilirubin was measured at inclusion and at days 2, 4, 7 and 14. The primary objective was to analyse the bilirubin at inclusion according to the 90-day mortality rate.
Results: The 90-day mortality rate was 33.8% (n = 272). The non-survivors were older, had higher Sepsis-related Organ Failure Assessment (SOFA) score and were more likely to have a medical diagnosis on admission than the survivors. At inclusion, the SOFA score without the liver score (10.3±2.9 vs. 9.0±3.0, p<0.0001) and the serum bilirubin levels (36.1±57.0 vs. 20.5±31.5 μmol/L, p<0.0001) were significantly higher in the non-survivors than in the survivors. Age, the hepatic SOFA score, the coagulation SOFA score, the arterial pH level, and the plateau pressure were independently associated with 90-day mortality in patients with ARDS.
Conclusion: Bilirubin used as a surrogate marker of hepatic dysfunction and measured early in the course of ARDS was associated with the 90-day mortality rate.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
