

The antiphospholipid syndrome: still an enigma
- PMID: 26637701
- PMCID: PMC4877624
- DOI: 10.1182/asheducation-2015.1.53
The antiphospholipid syndrome: still an enigma
Abstract
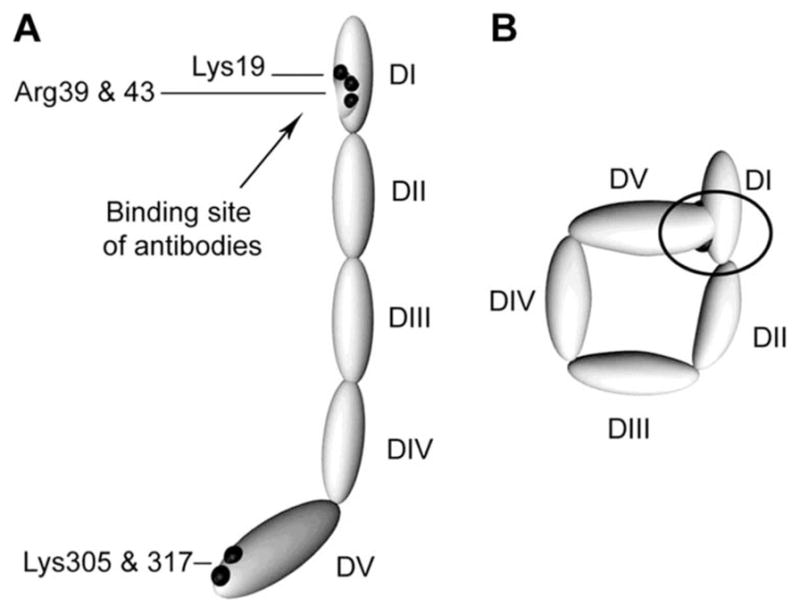
Antiphospholipid syndrome (APS) is defined by clinical manifestations that include thrombosis and/or fetal loss or pregnancy morbidity in patients with antiphospholipid antibodies (aPL). Antiphospholipid antibodies are among the most common causes of acquired thrombophilia, but unlike most of the genetic thrombophilias are associated with both venous and arterial thrombosis. Despite an abundance of clinical and basic research on aPL, a unified mechanism that explains their prothrombotic activity has not been defined; this may reflect the heterogeneity of aPL and/or the fact that they may influence multiple pro- and/or antithrombotic pathways. Antiphospholipid antibodies are directed primarily toward phospholipid binding proteins rather than phospholipid per se, with the most common antigenic target being β2-glycoprotein 1 (β2GPI) although antibodies against other targets such as prothrombin are well described. Laboratory diagnosis of aPL depends upon the detection of a lupus anticoagulant (LA), which prolongs phospholipid-dependent anticoagulation tests, and/or anticardiolipin and anti-β2-glycoprotein 1 antibodies. Indefinite anticoagulation remains the mainstay of therapy for thrombotic APS, although new strategies that may improve outcomes are emerging. Preliminary reports suggest caution in the use of direct oral anticoagulants in patients with APS-associated thrombosis. Based on somewhat limited evidence, aspirin and low molecular weight heparin are recommended for obstetrical APS. There remains a pressing need for better understanding of the pathogenesis of APS in humans, for identification of clinical and laboratory parameters that define patients at greatest risk for APS-related events, and for targeted treatment of this common yet enigmatic disorder.
© 2015 by The American Society of Hematology. All rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
Similar articles
-
Diagnosis and management of the antiphospholipid syndrome.Blood Rev. 2017 Nov;31(6):406-417. doi: 10.1016/j.blre.2017.07.006. Epub 2017 Jul 30. Blood Rev. 2017. PMID: 28784423 Free PMC article. Review.
-
The role of beta 2-glycoprotein I-dependent lupus anticoagulants in the pathogenesis of the antiphospholipid syndrome.Verh K Acad Geneeskd Belg. 2000;62(5):353-72. Verh K Acad Geneeskd Belg. 2000. PMID: 11144685 Review.
-
[Clinical significance of antiphospholipid antibodies].Rinsho Byori. 1998 Apr;46(4):297-302. Rinsho Byori. 1998. PMID: 9594618 Review. Japanese.
-
The value of IgA antiphospholipid testing for diagnosis of antiphospholipid (Hughes) syndrome in systemic lupus erythematosus.J Rheumatol. 2001 Dec;28(12):2637-43. J Rheumatol. 2001. PMID: 11764209
-
Novel diagnostic and therapeutic frontiers in thrombotic anti-phospholipid syndrome.Intern Emerg Med. 2017 Feb;12(1):1-7. doi: 10.1007/s11739-016-1596-2. Epub 2017 Jan 2. Intern Emerg Med. 2017. PMID: 28044251 Review.
Cited by
-
High prevalence of thrombophilic risk factors in patients with central retinal artery occlusion.Thromb J. 2023 Jul 28;21(1):81. doi: 10.1186/s12959-023-00525-z. Thromb J. 2023. PMID: 37507715 Free PMC article.
-
Diagnosis and management of the antiphospholipid syndrome.Blood Rev. 2017 Nov;31(6):406-417. doi: 10.1016/j.blre.2017.07.006. Epub 2017 Jul 30. Blood Rev. 2017. PMID: 28784423 Free PMC article. Review.
-
Hallux Partial Necrosis Associated with Antiphospholipid Syndrome: The Importance of Early Accurate Diagnosis.Life (Basel). 2023 Apr 13;13(4):1009. doi: 10.3390/life13041009. Life (Basel). 2023. PMID: 37109538 Free PMC article.
-
The antiphospholipid syndrome may induce non-thrombotic internal jugular vein stenosis: two cases report.BMC Neurol. 2021 Jan 7;21(1):9. doi: 10.1186/s12883-020-02035-1. BMC Neurol. 2021. PMID: 33413173 Free PMC article.
-
The well-defined antiphospholipid syndrome induced by COVID-19: a rare case report and review of the literature.Thromb J. 2024 Nov 8;22(1):99. doi: 10.1186/s12959-024-00669-6. Thromb J. 2024. PMID: 39516860 Free PMC article. Review.
References
-
- Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS) J Thromb Haemost. 2006;4(2):295–306. - PubMed
-
- Cervera R, Piette JC, Font J, et al. Antiphospholipid syndrome: clinical and immunologic manifestations and patterns of disease expression in a cohort of 1000 patients. Arthritis Rheum. 2002;46(4):1019–1027. - PubMed
-
- Asherson RA, Cervera R, de Groot PG, et al. Catastrophic antiphospho-lipid syndrome: international consensus statement on classification criteria and treatment guidelines. Lupus. 2003;12(7):530–534. - PubMed
-
- Cervera R, Serrano R, Pons-Estel GJ, et al. Morbidity and mortality in the antiphospholipid syndrome during a 10-year period: a multicentre prospective study of 1000 patients. Ann Rheum Dis. 2015;74(6):1011–1018. - PubMed
-
- Cervera R, Espinosa G. Update on the catastrophic antiphospholipid syndrome and the “CAPS Registry”. Semin Thromb Hemost. 2012;38(4):333–338. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous