

Ibrutinib as Initial Therapy for Patients with Chronic Lymphocytic Leukemia
- PMID: 26639149
- PMCID: PMC4722809
- DOI: 10.1056/NEJMoa1509388
Ibrutinib as Initial Therapy for Patients with Chronic Lymphocytic Leukemia
Abstract
Background: Chronic lymphocytic leukemia (CLL) primarily affects older persons who often have coexisting conditions in addition to disease-related immunosuppression and myelosuppression. We conducted an international, open-label, randomized phase 3 trial to compare two oral agents, ibrutinib and chlorambucil, in previously untreated older patients with CLL or small lymphocytic lymphoma.
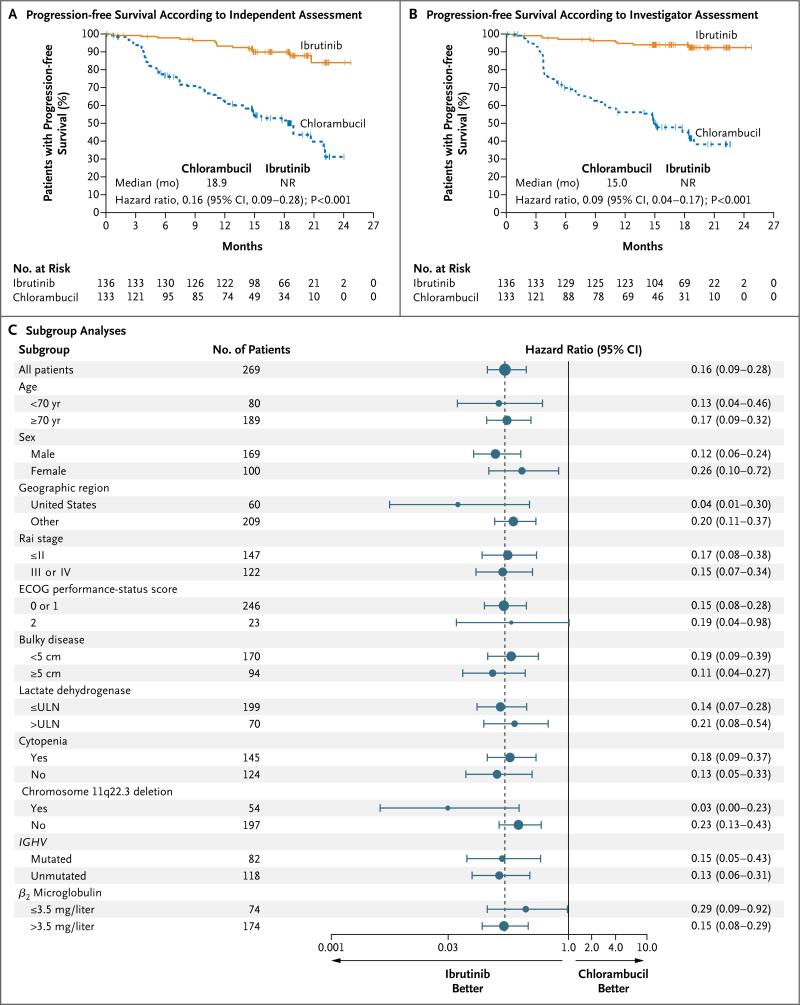
Methods: We randomly assigned 269 previously untreated patients who were 65 years of age or older and had CLL or small lymphocytic lymphoma to receive ibrutinib or chlorambucil. The primary end point was progression-free survival as assessed by an independent review committee.
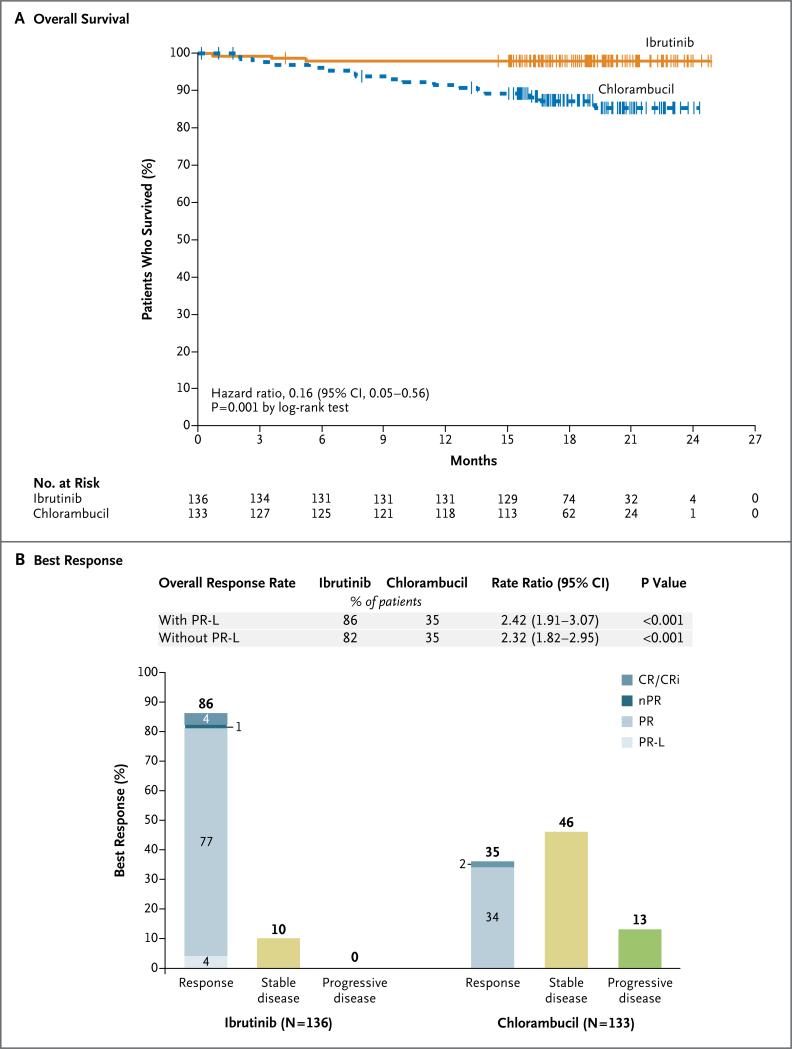
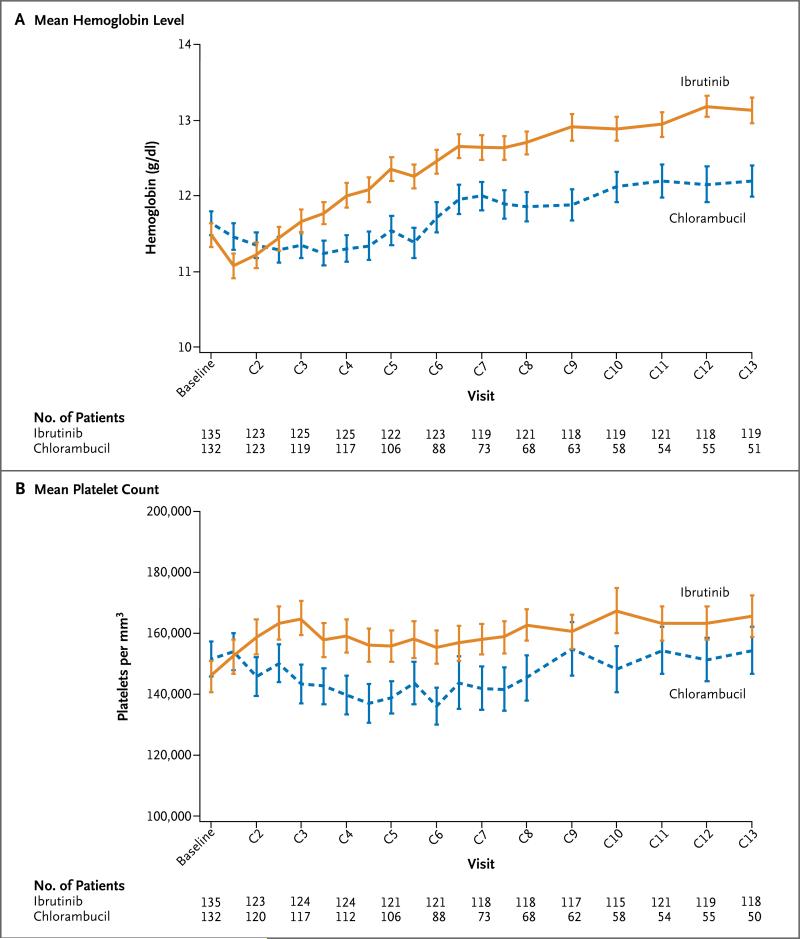
Results: The median age of the patients was 73 years. During a median follow-up period of 18.4 months, ibrutinib resulted in significantly longer progression-free survival than did chlorambucil (median, not reached vs. 18.9 months), with a risk of progression or death that was 84% lower with ibrutinib than that with chlorambucil (hazard ratio, 0.16; P<0.001). Ibrutinib significantly prolonged overall survival; the estimated survival rate at 24 months was 98% with ibrutinib versus 85% with chlorambucil, with a relative risk of death that was 84% lower in the ibrutinib group than in the chlorambucil group (hazard ratio, 0.16; P=0.001). The overall response rate was higher with ibrutinib than with chlorambucil (86% vs. 35%, P<0.001). The rates of sustained increases from baseline values in the hemoglobin and platelet levels were higher with ibrutinib. Adverse events of any grade that occurred in at least 20% of the patients receiving ibrutinib included diarrhea, fatigue, cough, and nausea; adverse events occurring in at least 20% of those receiving chlorambucil included nausea, fatigue, neutropenia, anemia, and vomiting. In the ibrutinib group, four patients had a grade 3 hemorrhage and one had a grade 4 hemorrhage. A total of 87% of the patients in the ibrutinib group are continuing to take ibrutinib.
Conclusions: Ibrutinib was superior to chlorambucil in previously untreated patients with CLL or small lymphocytic lymphoma, as assessed by progression-free survival, overall survival, response rate, and improvement in hematologic variables. (Funded by Pharmacyclics and others; RESONATE-2 ClinicalTrials.gov number, NCT01722487.).
Figures
Comment in
-
Ibrutinib increased survival more than chlorambucil in older patients with untreated chronic lymphocytic leukemia.Ann Intern Med. 2016 Apr 19;164(8):JC44. doi: 10.7326/ACPJC-2016-164-8-044. Ann Intern Med. 2016. PMID: 27089094 No abstract available.
-
Ibrutinib for Chronic Lymphocytic Leukemia.N Engl J Med. 2016 Apr 21;374(16):1594-5. doi: 10.1056/NEJMc1600328. N Engl J Med. 2016. PMID: 27096594 No abstract available.
-
Ibrutinib for Chronic Lymphocytic Leukemia.N Engl J Med. 2016 Apr 21;374(16):1592-3. doi: 10.1056/NEJMc1600328. N Engl J Med. 2016. PMID: 27096595 No abstract available.
-
Ibrutinib for Chronic Lymphocytic Leukemia.N Engl J Med. 2016 Apr 21;374(16):1593. doi: 10.1056/NEJMc1600328. N Engl J Med. 2016. PMID: 27096596 No abstract available.
-
Ibrutinib for Chronic Lymphocytic Leukemia.N Engl J Med. 2016 Apr 21;374(16):1593-4. doi: 10.1056/NEJMc1600328. N Engl J Med. 2016. PMID: 27096597 No abstract available.
References
-
- Eichhorst B, Dreyling M, Robak T, Montserrat E, Hallek M. Chronic lymphocytic leukemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2011;22(Suppl 6):vi50–vi54. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5–29. - PubMed
-
- Eichhorst BF, Busch R, Stilgenbauer S, et al. First-line therapy with fludarabine compared with chlorambucil does not re sult in a major benefit for elderly patients with advanced chronic lymphocytic leukemia. Blood. 2009;114:3382–91. - PubMed
-
- Hillmen P, Skotnicki AB, Robak T, et al. Alemtuzumab compared with chlorambucil as first-line therapy for chronic lymphocytic leukemia. J Clin Oncol. 2007;25:5616–23. - PubMed
-
- Knauf WU, Lissichkov T, Aldaoud A, et al. Phase III randomized study of bendamustine compared with chlorambucil in previously untreated patients with chronic lymphocytic leukemia. J Clin Oncol. 2009;27:4378–84. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases