

Cerebrospinal Fluid Aβ40 Improves the Interpretation of Aβ42 Concentration for Diagnosing Alzheimer's Disease
- PMID: 26640457
- PMCID: PMC4661235
- DOI: 10.3389/fneur.2015.00247
Cerebrospinal Fluid Aβ40 Improves the Interpretation of Aβ42 Concentration for Diagnosing Alzheimer's Disease
Abstract
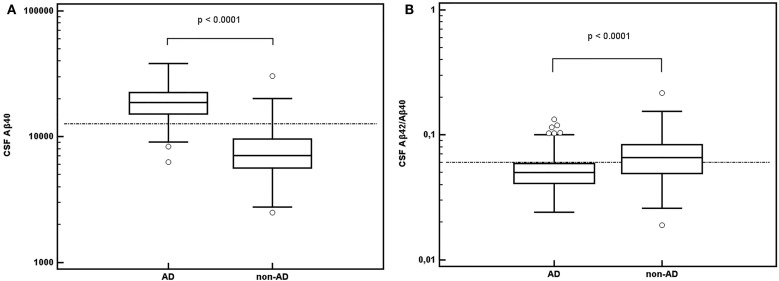
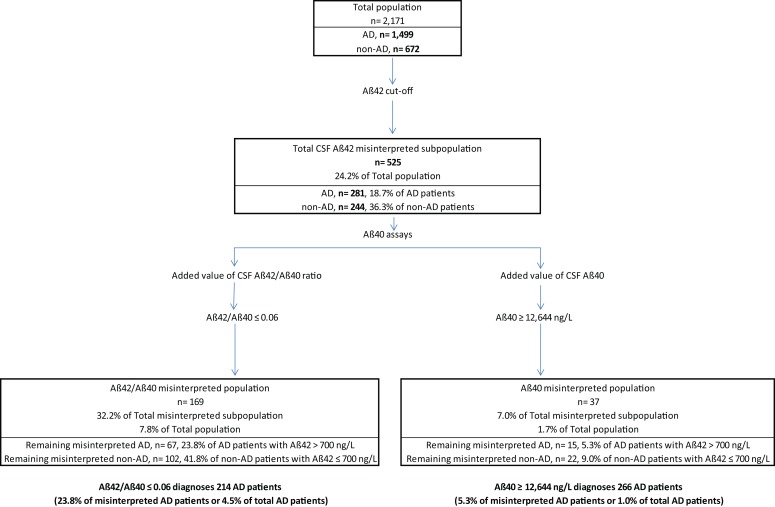
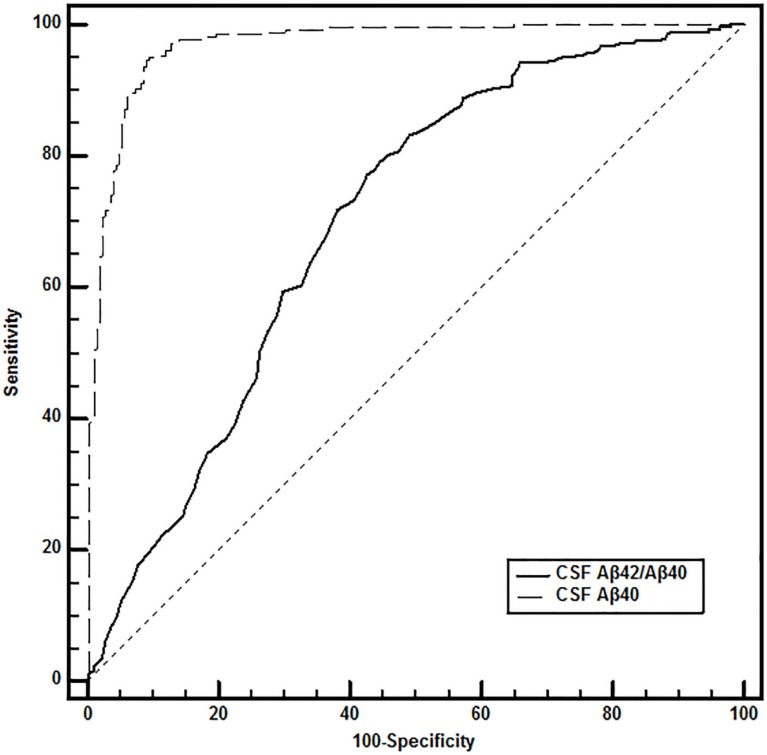
The combination of decreased amyloid β42 (Aβ42) and increased total tau proteins (T-Tau) and phosphorylated tau (P-Tau) in cerebrospinal fluid (CSF) has recently been considered as a biological diagnostic criterion of Alzheimer's disease (AD). Previous studies showed significant heterogeneity in CSF Aβ42 levels to discriminate AD from non-AD patients. It was also suggested that the CSF amyloid peptide β42/β40 ratio has better diagnostic performance than Aβ42 alone. The objective of the present study was to investigate the potential added value of determining CSF amyloid β40 peptide (Aβ40) for biological diagnosis of AD when CSF Aβ42 levels failed. CSF AD biomarkers were run in 2,171 samples from 1,499 AD and 672 non-AD patients. The following pathologic thresholds were used to define an AD-positive CSF biomarker profile: T-Tau ≥ 400 ng/L, P-Tau181 ≥ 60 ng/L, and Aβ42 ≤ 700 ng/L. CSF Aβ40 was assayed in AD patients with CSF Aβ42 levels above 700 ng/L and non-AD patients with CSF Aβ42 levels below 700 ng/L. CSF Aβ40 levels were higher in AD than non-AD patients. The receiver operator characteristic curves of CSF Aβ40 and the Aβ42/Aβ40 ratio defined AD cut-off values at 12,644 ng/L and 0.06, respectively. In AD patients with non-pathological CSF Aβ42, CSF Aβ40 concentration was able to correct 76.2% of cases when expressed as CSF Aβ42/Aβ40 ratio and 94.7% of cases when used alone. Using CSF Aβ42 and then CSF Aβ40, the percentage of misinterpreted AD patients fell to 1.0%. CSF Aβ40 concentration improved interpretation of Aβ42 level for the diagnosis of AD. CSF Aβ40 alone showed better diagnostic performance than the amyloid peptide Aβ42/Aβ40 ratio. The added value of determining CSF Aβ40 in AD diagnosis now needs confirming in a cohort of definite AD patients and to be completed with novel amyloid cascade biomarkers.
Keywords: Alzheimer; Aβ40; Aβ42; cerebrospinal fluid; dementia.
Figures
References
-
- McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR, Jr, Kawas CH, et al. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement (2011) 7(3):263–9. 10.1016/j.jalz.2011.03.005 - DOI - PMC - PubMed
-
- Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement (2011) 7(3):270–9. 10.1016/j.jalz.2011.03.008 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous