

Adjunctive Corticotherapy for Community Acquired Pneumonia: A Systematic Review and Meta-Analysis
- PMID: 26641253
- PMCID: PMC4671611
- DOI: 10.1371/journal.pone.0144032
Adjunctive Corticotherapy for Community Acquired Pneumonia: A Systematic Review and Meta-Analysis
Abstract
Background: Community-acquired pneumonia (CAP) induces lung and systemic inflammation, leading to high morbidity and mortality. We systematically reviewed the risks and benefits of adjunctive corticotherapy in the management of patients with CAP.
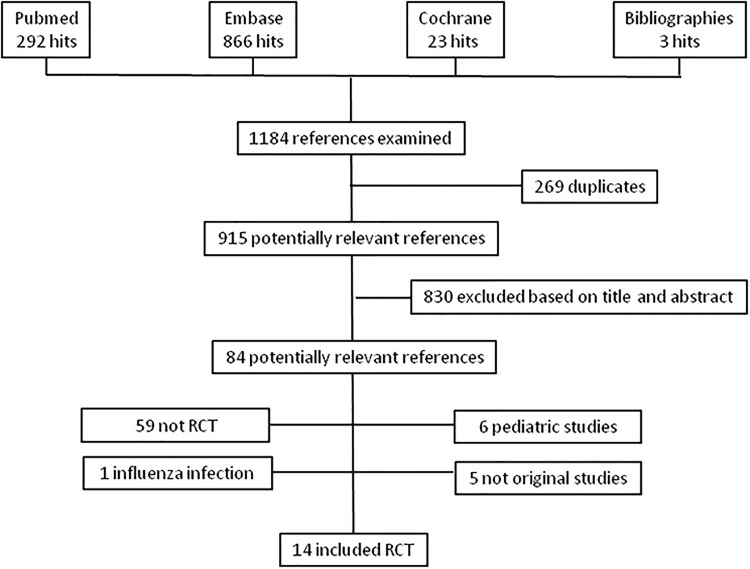
Methods: We systematically searched Pubmed, Embase and the Cochrane Library for randomized controlled trials comparing adjunctive corticotherapy and antimicrobial therapy with antimicrobial therapy alone in patients with CAP. The primary outcome was 30-day mortality. Secondary outcomes were length of hospital stay, time to clinical stability and severe complications.
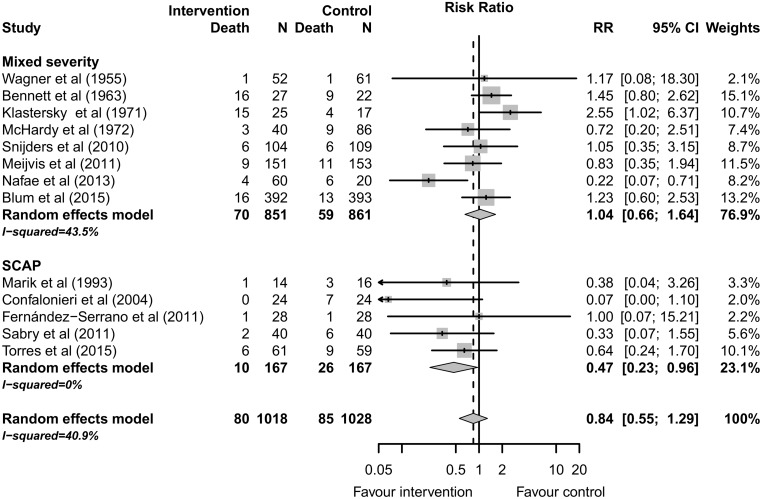
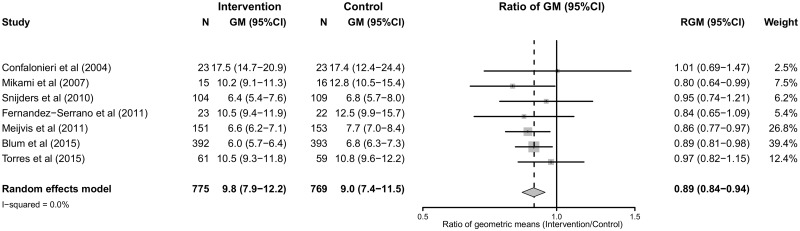
Results: 14 trials (2077 patients) were included. The reported 30-day mortality was 7.9% (80/1018) among patients treated with adjunctive corticotherapy versus 8.3% (85/1028) among patients treated with antimicrobial therapy alone (RR 0.84; 95%CI 0.55 to1.29). Adjunctive corticotherapy was associated with a reduction of severe complications (RR 0.36; 95%CI 0.23 to 0.56), a shorter length of stay (9.0 days; 95%CI 7.6 to 10.7 vs 10.6 days; 95%CI 7.4 to 15.3) and a shorter time to clinical stability (3.3 days; 95% CI 2.8 to 4.1 vs 4.3 days; 95%CI 3.6 to 5.1). The risk of hyperglycemia was higher among patients treated with adjunctive corticotherapy (RR 1.59; 95%CI 1.06 to 2.38), whereas the risk of gastro-intestinal bleeding was similar (RR 0.83; 95%CI 0.35 to 1.93). In the subgroup analysis based on CAP severity, a survival benefit was found among patients with severe CAP (RR 0.47; 95%CI 0.23 to 0.96).
Conclusion: Adjunctive corticotherapy is associated with a reduction of length of stay, time to clinical stability, and severe complications among patients with CAP, but the effect on mortality remains uncertain.
Conflict of interest statement
Figures
References
-
- Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385(9963):117–71. Epub 2014/12/23. doi: S0140-6736(14)61682-2 [pii] 10.1016/S0140-6736(14)61682-2 - DOI - PMC - PubMed
-
- Ewig S, Birkner N, Strauss R, Schaefer E, Pauletzki J, Bischoff H, et al. New perspectives on community-acquired pneumonia in 388 406 patients. Results from a nationwide mandatory performance measurement programme in healthcare quality. Thorax. 2009;64(12):1062–9. Epub 2009/05/21. doi: thx.2008.109785 [pii] 10.1136/thx.2008.109785 . - DOI - PMC - PubMed
-
- Walden AP, Clarke GM, McKechnie S, Hutton P, Gordon AC, Rello J, et al. Patients with community acquired pneumonia admitted to European intensive care units: an epidemiological survey of the GenOSept cohort. Crit Care. 2014;18(2):R58. Epub 2014/04/03. doi: cc13812 [pii] 10.1186/cc13812 - DOI - PMC - PubMed
-
- Laterre PF, Garber G, Levy H, Wunderink R, Kinasewitz GT, Sollet JP, et al. Severe community-acquired pneumonia as a cause of severe sepsis: data from the PROWESS study. Crit Care Med. 2005;33(5):952–61. Epub 2005/05/14. doi: 00003246-200505000-00006 [pii]. . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
