

Clinical Correlates of Mass Effect in Autosomal Dominant Polycystic Kidney Disease
- PMID: 26641645
- PMCID: PMC4671651
- DOI: 10.1371/journal.pone.0144526
Clinical Correlates of Mass Effect in Autosomal Dominant Polycystic Kidney Disease
Abstract
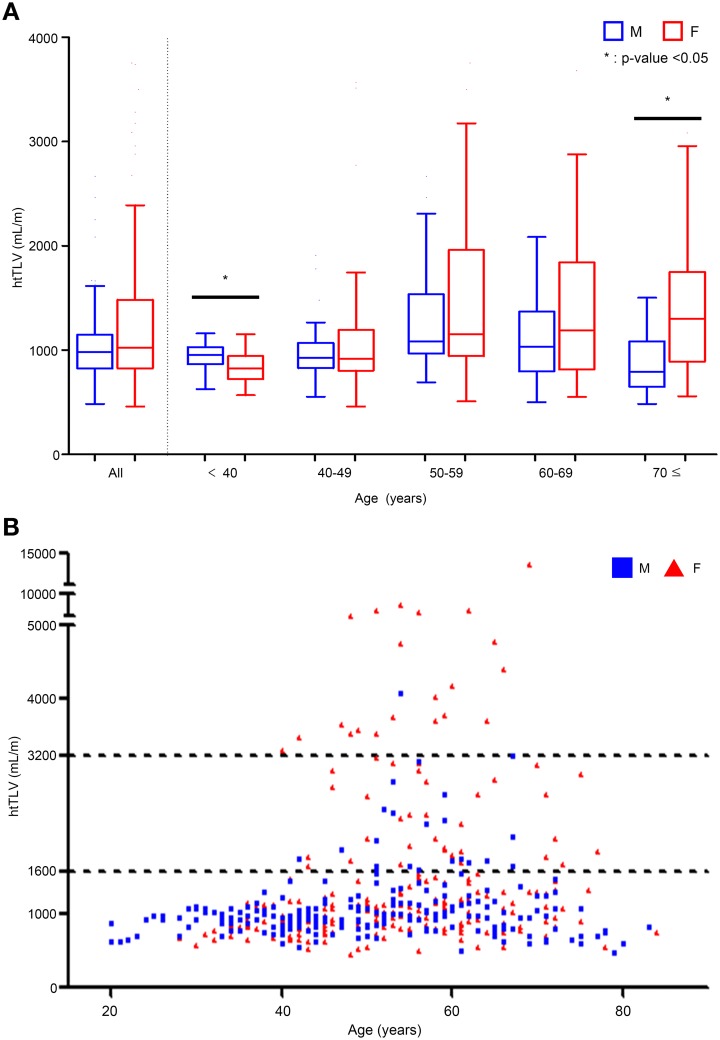
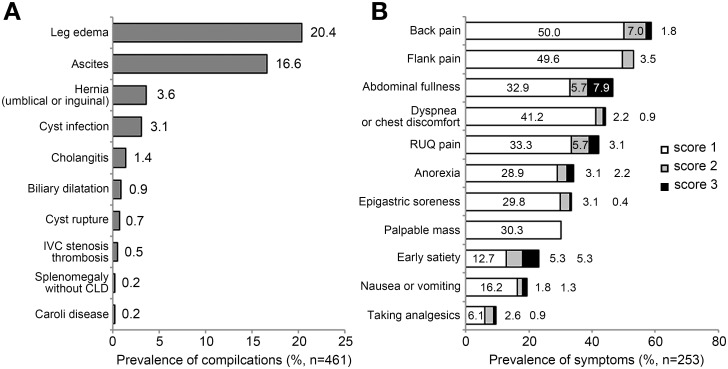
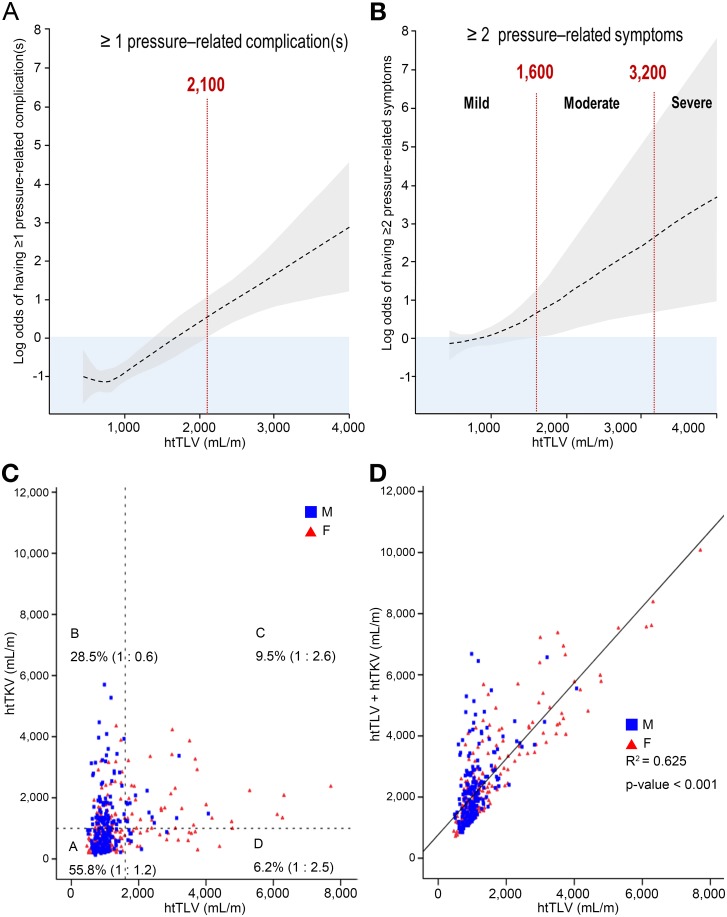
Mass effect from polycystic kidney and liver enlargement can result in significant clinical complications and symptoms in autosomal dominant polycystic kidney disease (ADPKD). In this single-center study, we examined the correlation of height-adjusted total liver volume (htTLV) and total kidney volume (htTKV) by CT imaging with hepatic complications (n = 461) and abdominal symptoms (n = 253) in patients with ADPKD. "Mass-effect" complications were assessed by review of medical records and abdominal symptoms, by a standardized research questionnaire. Overall, 91.8% of patients had 4 or more liver cysts on CT scans. Polycystic liver disease (PLD) was classified as none or mild (htTLV < 1,600 mL/m); moderate (1,600 ≤ htTLV <3,200 mL/m); and severe (htTLV ≥ 3,200 mL/m). The prevalence of moderate and severe PLD in our patient cohort was 11.7% (n = 54/461) and 4.8% (n = 22/461), respectively, with a female predominance in both the moderate (61.1%) and severe (95.5%) PLD groups. Pressure-related complications such as leg edema (20.4%), ascites (16.6%), and hernia (3.6%) were common, and patients with moderate to severe PLD exhibited a 6-fold increased risk (compared to no or mild PLD) for these complications in multivariate analysis. Similarly, abdominal symptoms including back pain (58.8%), flank pain (53.1%), abdominal fullness (46.5%), and dyspnea/chest-discomfort (44.3%) were very common, and patients with moderate to severe PLD exhibited a 5-fold increased risk for these symptoms. Moderate to severe PLD is a common and clinically important problem in ~16% of patients with ADPKD who may benefit from referral to specialized centers for further management.
Conflict of interest statement
Figures
References
-
- Chauveau D, Fakhouri F, Grünfeld JP. Liver involvement in autosomal-dominant polycystic kidney disease: therapeutic dilemma. J Am Soc Nephrol 2000;11:1767–1775. - PubMed
-
- Bae KT, Zhu F, Chapman AB, Torres VE, Grantham JJ, Guay-Woodford LM, et al. Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease (CRISP): Magnetic resonance imaging evaluation of hepatic cysts in early autosomal-dominant polycystic kidney disease: the Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease cohort. Clin J Am Soc Nephrol 2006;1:64–69. - PubMed
-
- Everson GT, Taylor MR. Management of polycystic liver disease. Curr Gastroenterol Rep 2005;7: 19–25. - PubMed
-
- Arnold HL, Harrison SA. New advances in evaluation and management of patients with polycystic liver disease. Am J Gastroenterol 2005;100: 2569–2582. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
