

Amikacin Pharmacokinetics/Pharmacodynamics in a Novel Hollow-Fiber Mycobacterium abscessus Disease Model
- PMID: 26643339
- PMCID: PMC4775936
- DOI: 10.1128/AAC.02282-15
Amikacin Pharmacokinetics/Pharmacodynamics in a Novel Hollow-Fiber Mycobacterium abscessus Disease Model
Abstract
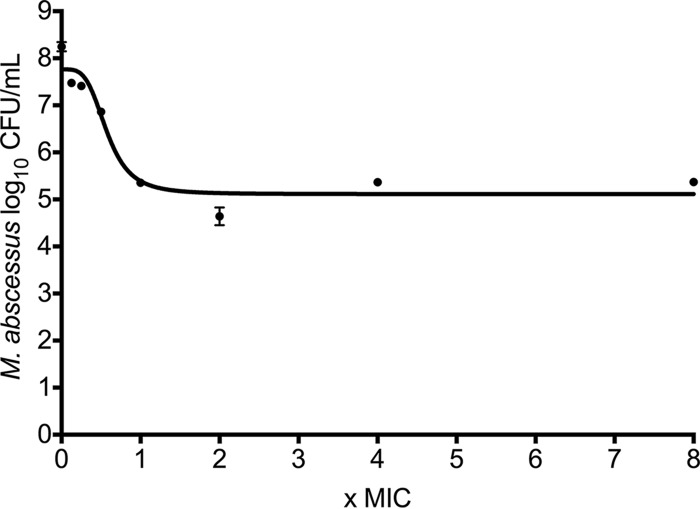
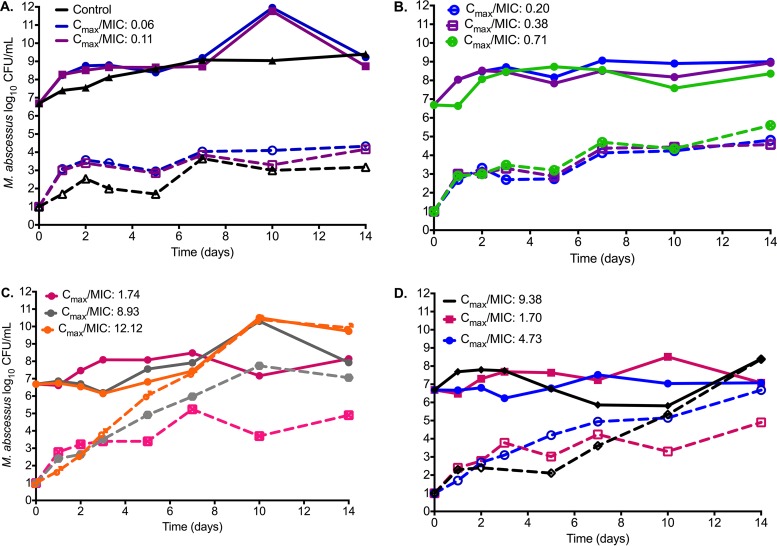
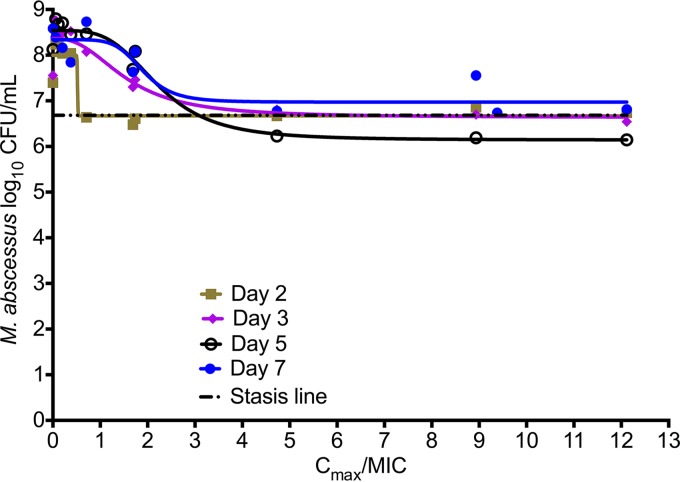
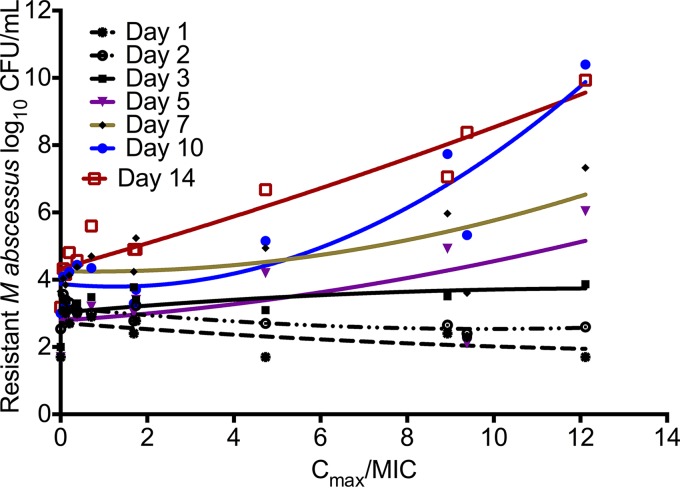
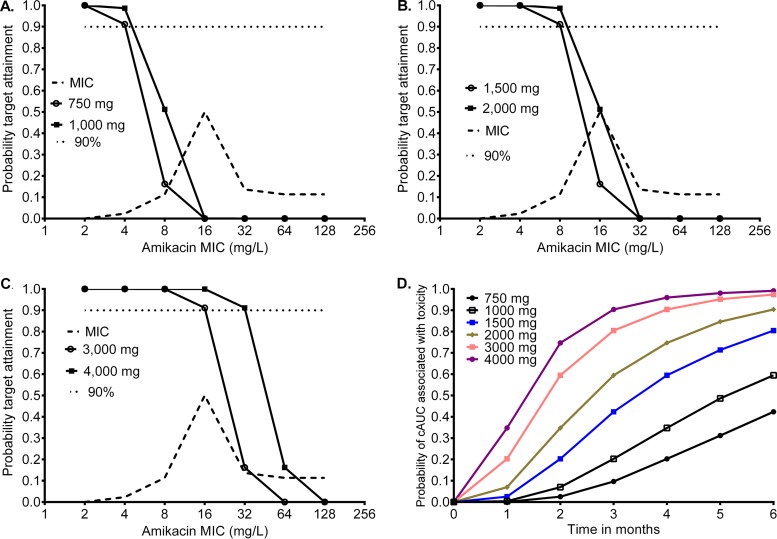
The treatment of pulmonary Mycobacterium abscessus disease is associated with very high failure rates and easily acquired drug resistance. Amikacin is the key drug in treatment regimens, but the optimal doses are unknown. No good preclinical model exists to perform formal pharmacokinetics/pharmacodynamics experiments to determine these optimal doses. We developed a hollow-fiber system model of M. abscessus disease and studied amikacin exposure effects and dose scheduling. We mimicked amikacin human pulmonary pharmacokinetics. Both amikacin microbial kill and acquired drug resistance were linked to the peak concentration-to-MIC ratios; the peak/MIC ratio associated with 80% of maximal kill (EC80) was 3.20. However, on the day of the most extensive microbial kill, the bacillary burden did not fall below the starting inoculum. We performed Monte Carlo simulations of 10,000 patients with pulmonary M. abscessus infection and examined the probability that patients treated with one of 6 doses from 750 mg to 4,000 mg would achieve or exceed the EC80. We also examined these doses for the ability to achieve a cumulative area under the concentration-time curve of 82,232 mg · h/liter × days, which is associated with ototoxicity. The standard amikacin doses of 750 to 1,500 mg a day achieved the EC80 in ≤ 21% of the patients, while a dose of 4 g/day achieved this in 70% of the patients but at the cost of high rates of ototoxicity within a month or two. The susceptibility breakpoint was an MIC of 8 to 16 mg/liter. Thus, amikacin, as currently dosed, has limited efficacy against M. abscessus. It is urgent that different antibiotics be tested using our preclinical model and new regimens developed.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, Holland SM, Horsburgh R, Huitt G, Iademarco MF, Iseman M, Olivier K, Ruoss S, von Reyn CF, Wallace RJ Jr, Winthrop K, ATS Mycobacterial Diseases Subcommittee, American Thoracic Society, Infectious Diseases Society of America. 2007. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med 175:367–416. doi:10.1164/rccm.200604-571ST. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
