

Screening and treatment of maternal genitourinary tract infections in early pregnancy to prevent preterm birth in rural Sylhet, Bangladesh: a cluster randomized trial
- PMID: 26643558
- PMCID: PMC4672554
- DOI: 10.1186/s12884-015-0724-8
Screening and treatment of maternal genitourinary tract infections in early pregnancy to prevent preterm birth in rural Sylhet, Bangladesh: a cluster randomized trial
Abstract
Background: Approximately half of preterm births are attributable to maternal infections, which are commonly undetected and untreated in low-income settings. Our primary aim is to determine the impact of early pregnancy screening and treatment of maternal genitourinary tract infections on the incidence of preterm live birth in Sylhet, Bangladesh. We will also assess the effect on other adverse pregnancy outcomes, including preterm birth (stillbirth and live birth), late miscarriage, maternal morbidity, and early onset neonatal sepsis.
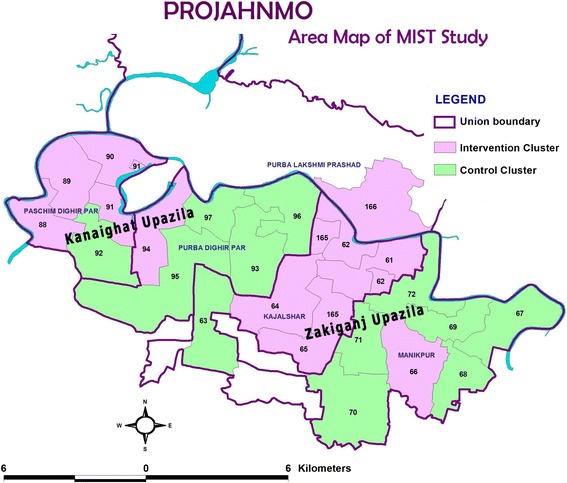
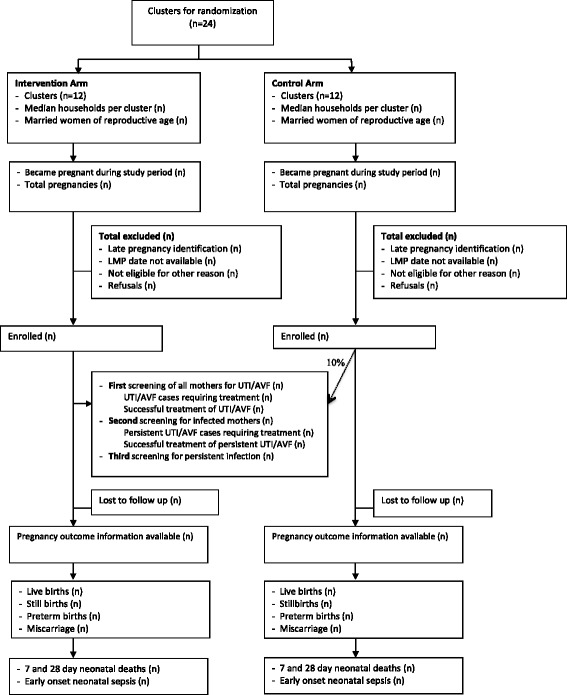
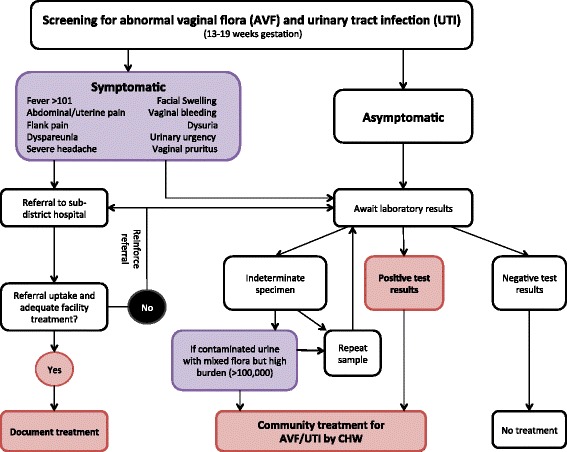
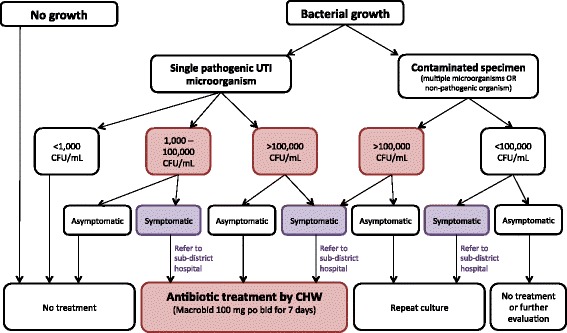
Methods/design: We are conducting a cluster randomized controlled trial that will enroll 10,000 pregnant women in Sylhet district in rural northeastern Bangladesh. Twenty-four clusters, each with ~4000 population (120 pregnant women/year) and served by a community health worker (CHW), are randomized to: 1) the control arm, which provides routine antenatal and postnatal home-based care, or 2) the intervention arm, which includes routine antenatal and postnatal home-based care plus screening and treatment of pregnant women between 13 and 19 weeks of gestation for abnormal vaginal flora (AVF) and urinary tract infection (UTI). CHWs conduct monthly pregnancy surveillance, make 2 antenatal and 4 postnatal home visits for all enrolled pregnant women and newborns, and refer mothers or newborns with symptoms of serious illness to the government sub-district hospital. In the intervention clusters, CHWs perform home-based screening of AVF and UTI. Self-collected vaginal swabs are plated on slides, which are Gram stained and Nugent scored. Women with AVF (Nugent score ≥4) are treated with oral clindamycin, rescreened and retreated, if needed, after 3 weeks. Urine culture is performed and UTI treated with nitrofurantoin. Repeat urine culture is performed after 1 week for test of cure. Gestational age is determined by maternal report of last menstrual period at study enrollment using prospectively completed study calendars, and in a subset by early (<20 week) ultrasound. CHWs prospectively collect data on all pregnancy outcomes, maternal and neonatal morbidity and mortality.
Implications/discussion: Findings will enhance our understanding of the burden of AVF and UTI in rural Bangladesh, the impact of a maternal screening-treatment program for genitourinary tract infections on perinatal health, and help formulate public health recommendations for infection screening in pregnancy in low-resource settings.
Trial registration: The study was registered on ClinicalTrials.gov:NCT01572532 on December 15, 2011. The study was funded by NICHD: R01HD066156 .
Figures
References
-
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, Adler A, Vera Garcia C, Rohde S, Say L, Lawn JE. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379:2162–72. doi: 10.1016/S0140-6736(12)60820-4. - DOI - PubMed
-
- Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, Cousens S, Mathers C, Black RE. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015;385:430–40. doi: 10.1016/S0140-6736(14)61698-6. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
