

Practice guideline: Idiopathic normal pressure hydrocephalus: Response to shunting and predictors of response: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology
- PMID: 26644048
- PMCID: PMC4676757
- DOI: 10.1212/WNL.0000000000002193
Practice guideline: Idiopathic normal pressure hydrocephalus: Response to shunting and predictors of response: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology
Erratum in
-
Practice Guideline: Idiopathic normal pressure hydrocephalus: Response to shunting and predictors of response: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology.Neurology. 2016 Feb 23;86(8):793. doi: 10.1212/WNL.0000000000002432. Neurology. 2016. PMID: 26903492 Free PMC article. No abstract available.
Abstract
Objective: We evaluated evidence for utility of shunting in idiopathic normal pressure hydrocephalus (iNPH) and for predictors of shunting effectiveness.
Methods: We identified and classified relevant published studies according to 2004 and 2011 American Academy of Neurology methodology.
Results: Of 21 articles, we identified 3 Class I articles.
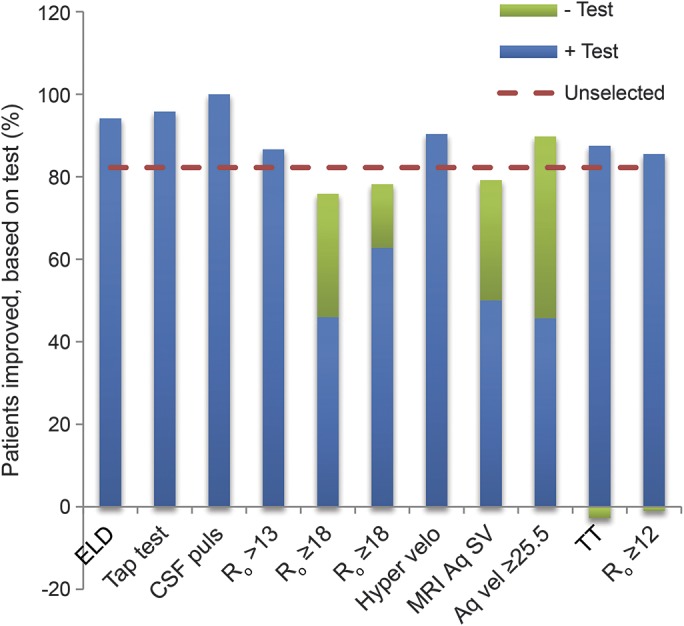
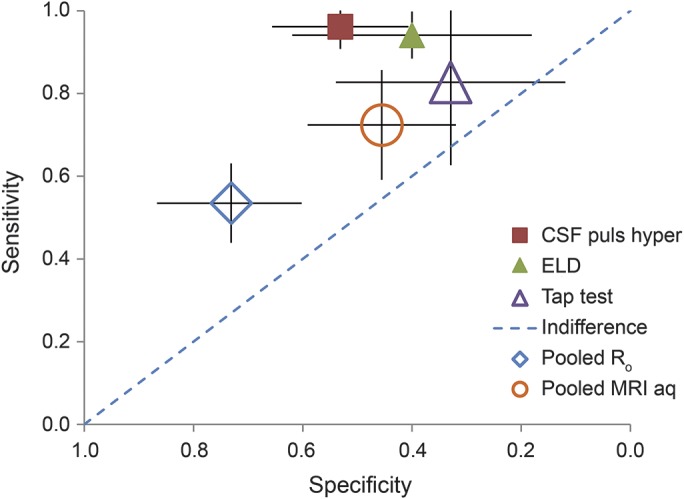
Conclusions: Shunting is possibly effective in iNPH (96% chance subjective improvement, 83% chance improvement on timed walk test at 6 months) (3 Class III). Serious adverse event risk was 11% (1 Class III). Predictors of success included elevated Ro (1 Class I, multiple Class II), impaired cerebral blood flow reactivity to acetazolamide (by SPECT) (1 Class I), and positive response to either external lumbar drainage (1 Class III) or repeated lumbar punctures. Age may not be a prognostic factor (1 Class II). Data are insufficient to judge efficacy of radionuclide cisternography or aqueductal flow measurement by MRI.
Recommendations: Clinicians may choose to offer shunting for subjective iNPH symptoms and gait (Level C). Because of significant adverse event risk, risks and benefits should be carefully weighed (Level B). Clinicians should inform patients with iNPH with elevated Ro and their families that they have an increased chance of responding to shunting compared with those without such elevation (Level B). Clinicians may counsel patients with iNPH and their families that (1) positive response to external lumbar drainage or to repeated lumbar punctures increases the chance of response to shunting, and (2) increasing age does not decrease the chance of shunting being successful (both Level C).
© 2015 American Academy of Neurology.
Figures
References
-
- Hakim S, Adams RD. The special clinical problem of symptomatic hydrocephalus with normal cerebrospinal fluid pressure: observations on cerebrospinal fluid hydrodynamics. J Neurol Sci 1965;2:307–327. - PubMed
-
- Brean A, Eide PK. Prevalence of probable idiopathic normal pressure hydrocephalus in a Norwegian population. Acta Neurol Scand 2008;118:48–53. - PubMed
-
- Ishikawa M. Clinical guidelines for idiopathic normal pressure hydrocephalus. Neurol Med Chir 2004;44:222–223. - PubMed
-
- Hebb AO, Cusimano MD. Idiopathic normal pressure hydrocephalus: a systematic review of diagnosis and outcome. Neurosurgery 2001;49:1166–1184; discussion 1184−1186. - PubMed
-
- Kahlon B, Sjunnesson J, Rehncrona S. Long-term outcome in patients with suspected normal pressure hydrocephalus. Neurosurgery 2007;60:327–332; discussion 332. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials