

Histological changes of kidney in diabetic nephropathy
- PMID: 26644877
- PMCID: PMC4650785
Histological changes of kidney in diabetic nephropathy
Abstract
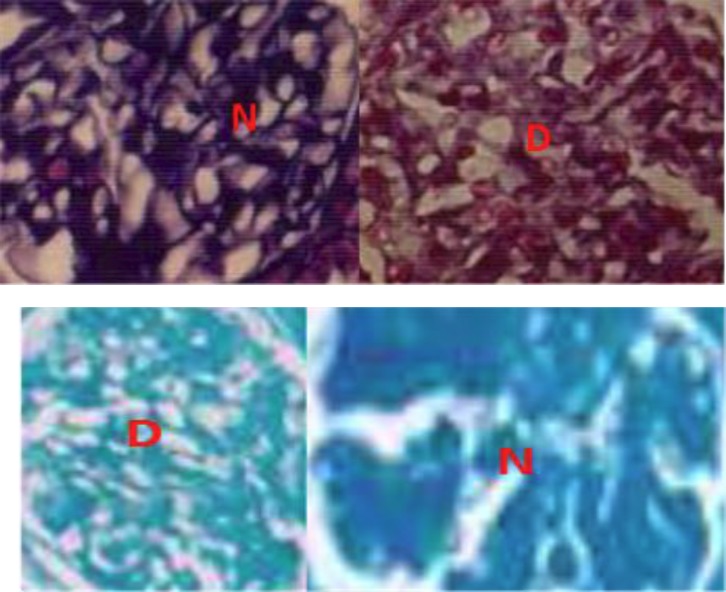
Diabetes mellitus is the most common cause of chronic renal disorders and end-stage kidney disease in developed countries. It is the major cause of dialysis and transplantation. Failure in renal function causes wide disorders in the body. Diabetes results in wide range of alterations in the renal tissue. It is believed that early histological changes in diabetic nephropathy are detectable 2 years after diabetes is diagnosed. The glomerular alterations are the most important lesions in the diabetic nephropathy (DN). The Renal Pathology Society provides a new pathological classification for the detection of histopathology of DN. It divides diabetic nephropathy into four hierarchical glomerular lesions. Alloxan or streptozotocin induced diabetic rat is the one most widely used specie to study DN. Histological changes in the rat DN closely resemble the human disease and the most information of this review was obtained through the study of rat DN. All cell types of the kidney such as mesangial cells, podocytes and tubulointerstitial cells are liable to be affected in the event of DN. Severity of renal lesions is associated to the clinical aspect of renal outcome, but the aim of this article was only to review the histological changes of kidney in diabetes mellitus.
Keywords: Diabetes mellitus; Histological changes; Nephropathy.
Figures





References
Publication types
LinkOut - more resources
Full Text Sources