

Conservative mastectomies and immediate reconstruction with the use of ADMs
- PMID: 26644999
- PMCID: PMC4647009
- DOI: 10.3978/j.issn.2227-684X.2015.02.03
Conservative mastectomies and immediate reconstruction with the use of ADMs
Abstract
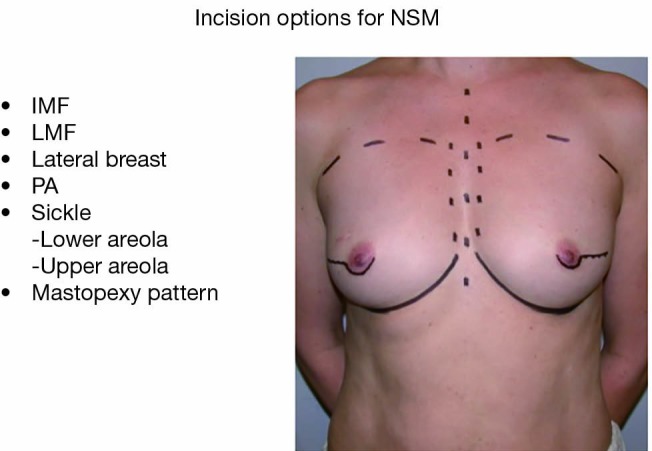
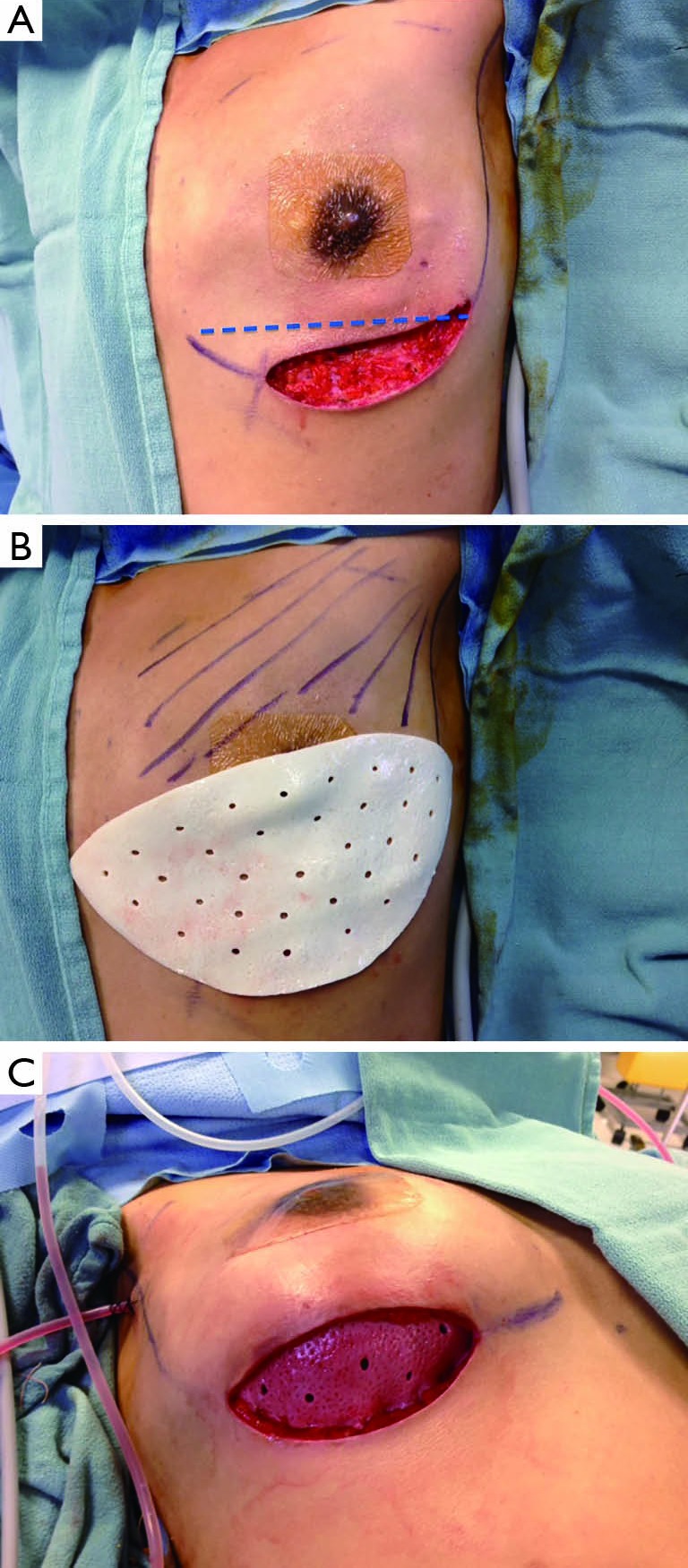
Background: In recent years, a novel approach to immediate breast reconstruction has been introduced with the advent of acellular dermal matrix (ADM). In the setting of conservative mastectomies where the native skin envelope is preserved, placement of ADM at the lower pole in continuity with the pectoralis major muscle (PMM) provides additional support, allowing direct-to-implant breast reconstruction. The following manuscript presents the senior author's experience with ADM-assisted reconstruction and provides a detailed description of surgical technique along with a comprehensive discussion of patient selection and potential complications.
Methods: A retrospective chart review of patients undergoing direct-to-implant breast reconstruction following skin sparing or nipple sparing mastectomy with the use of ADM (AlloDerm; LifeCell Corp., Branchburg, USA) was conducted at Women's College Hospital in Toronto over a 5-year period [2008-2013]. Demographic data, previous radiation therapy and post-operative complications were recorded.
Results: A total of 72 patients representing 119 breasts were identified. Average follow-up was 16 months (range, 3-51 months). Twenty-seven complications were recorded for a complication rate of 22.7% (27/119). Complications included six cases of capsular contracture (Baker III/IV), five cases of red skin syndrome, four cases of rippling, three cases of dehiscence and two cases of seroma. Overall, direct-to-implant reconstruction was successfully completed in 97.5% of breasts (116/119). One case of infection was treated with explantation and conversion to autogenous reconstruction. Two breasts with tissue necrosis or dehiscence had the implants removed and replaced with tissue expanders. Overall reoperation rate was 9.7% (7/72 patients).
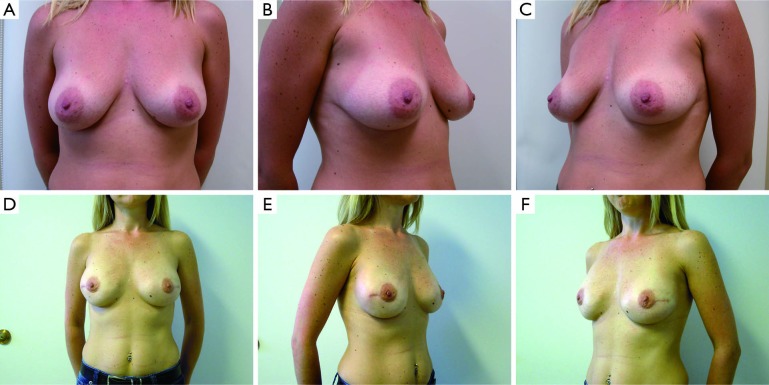
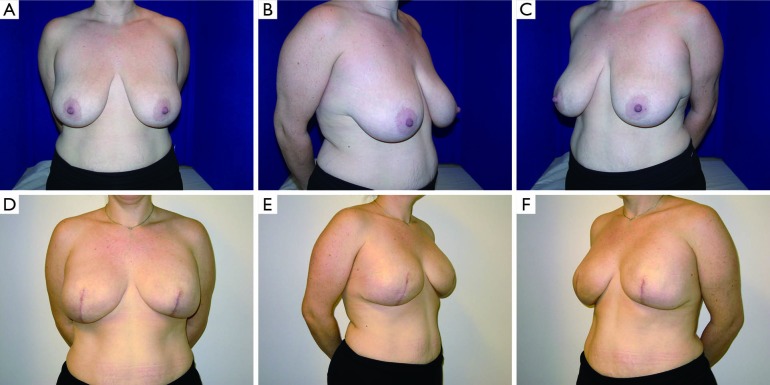
Conclusions: ADM assisted direct-to-implant breast reconstruction has been shown to be a safe option for women who are candidates for skin sparing or nipple sparing mastectomies. Judicious patient selection, effective collaboration between the oncologic and reconstructive surgeon, careful evaluation of post-mastectomy skin flaps and precise surgical technique are paramount to the success of this technique.
Keywords: Acellular dermis; breast reconstruction; conservative mastectomy; direct to implant; implant-based.
Conflict of interest statement
Figures

References
-
- Salzberg CA. Focus on technique: one-stage implant-based breast reconstruction. Plast Reconstr Surg 2012;130:95S-103S. - PubMed
-
- Vardanian AJ, Clayton JL, Roostaeian J, et al. Comparison of implant-based immediate breast reconstruction with and without acellular dermal matrix. Plast Reconstr Surg 2011;128:403e-10e. - PubMed
-
- Salzberg CA. Direct-to-implant breast reconstruction. Clin Plast Surg 2012;39:119-26. - PubMed
-
- Davidge KM, Brown M, Morgan P, et al. Processes of care in autogenous breast reconstruction with pedicled TRAM flaps: expediting postoperative discharge in an ambulatory setting. Plast Reconstr Surg 2013;132:339e-44e. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources