

Comparative benefits and harms of second generation antidepressants and cognitive behavioral therapies in initial treatment of major depressive disorder: systematic review and meta-analysis
- PMID: 26645251
- PMCID: PMC4673103
- DOI: 10.1136/bmj.h6019
Comparative benefits and harms of second generation antidepressants and cognitive behavioral therapies in initial treatment of major depressive disorder: systematic review and meta-analysis
Abstract
Study question: What are the benefits and harms of second generation antidepressants and cognitive behavioral therapies (CBTs) in the initial treatment of a current episode of major depressive disorder in adults?
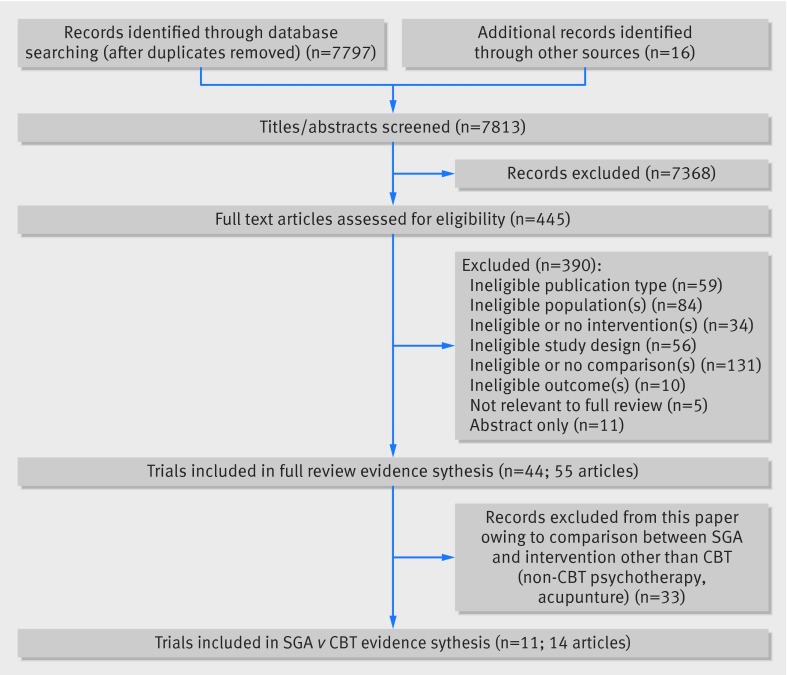
Methods: This was a systematic review including qualitative assessment and meta-analyses using random and fixed effects models. Medline, Embase, the Cochrane Library, the Allied and Complementary Medicine Database, PsycINFO, and the Cumulative Index to Nursing and Allied Health Literature were searched from January 1990 through January 2015. The 11 randomized controlled trials included compared a second generation antidepressant CBT. Ten trials compared antidepressant monotherapy with CBT alone; three compared antidepressant monotherapy with antidepressant plus CBT.
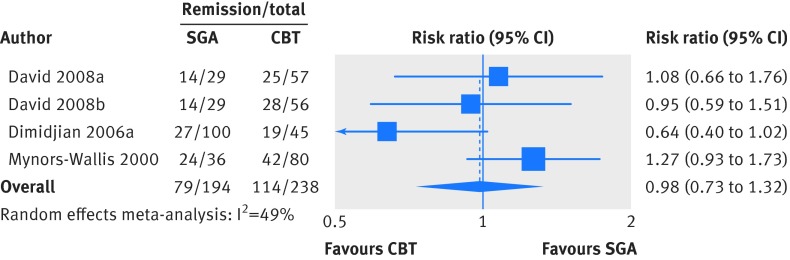
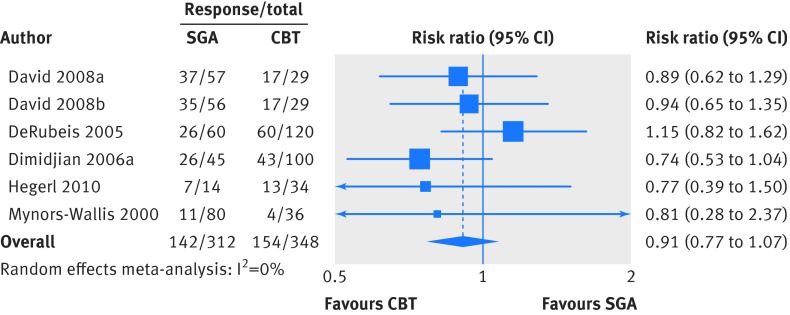
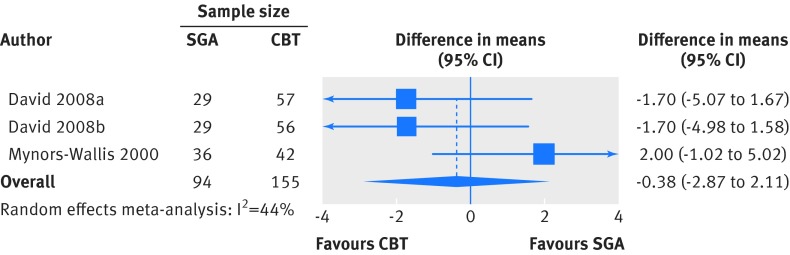
Summary answer and limitations: Meta-analyses found no statistically significant difference in effectiveness between second generation antidepressants and CBT for response (risk ratio 0.91, 0.77 to 1.07), remission (0.98, 0.73 to 1.32), or change in 17 item Hamilton Rating Scale for Depression score (weighted mean difference, -0.38, -2.87 to 2.10). Similarly, no significant differences were found in rates of overall study discontinuation (risk ratio 0.90, 0.49 to 1.65) or discontinuation attributable to lack of efficacy (0.40, 0.05 to 2.91). Although more patients treated with a second generation antidepressant than receiving CBT withdrew from studies because of adverse events, the difference was not statistically significant (risk ratio 3.29, 0.42 to 25.72). No conclusions could be drawn about other outcomes because of lack of evidence. Results should be interpreted cautiously given the low strength of evidence for most outcomes. The scope of this review was limited to trials that enrolled adult patients with major depressive disorder and compared a second generation antidepressant with CBT, and many of the included trials had methodological shortcomings that may limit confidence in some of the findings.
What this study adds: Second generation antidepressants and CBT have evidence bases of benefits and harms in major depressive disorder. Available evidence suggests no difference in treatment effects of second generation antidepressants and CBT, either alone or in combination, although small numbers may preclude detection of small but clinically meaningful differences. Funding, competing interests, data sharing This project was funded under contract from the Agency for Healthcare Research and Quality by the RTI-UNC Evidence-based Practice Center. Detailed methods and additional information are available in the full report, available at http://effectivehealthcare.ahrq.gov/.
© Amick et al 2015.
Conflict of interest statement
Competing interests: The authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Cognitive behavioural therapy or antidepressants for acute depression?BMJ. 2015 Dec 8;351:h6315. doi: 10.1136/bmj.h6315. BMJ. 2015. PMID: 26646303 No abstract available.
-
The problem of accessing psychotherapies for depression in the UK.BMJ. 2016 Jan 13;352:i119. doi: 10.1136/bmj.i119. BMJ. 2016. PMID: 26762309 No abstract available.
-
Antidepressants are addictive and increase the risk of relapse.BMJ. 2016 Feb 10;352:i574. doi: 10.1136/bmj.i574. BMJ. 2016. PMID: 26864863 No abstract available.
-
Authors' reply to Gøtzsche and Hamilton.BMJ. 2016 Feb 10;352:i617. doi: 10.1136/bmj.i617. BMJ. 2016. PMID: 26864955 No abstract available.
-
Patients in trials of antidepressants are not typical of those in everyday practice.BMJ. 2016 Feb 10;352:i577. doi: 10.1136/bmj.i577. BMJ. 2016. PMID: 26865187 No abstract available.
-
Second-generation antidepressants and cognitive-behavioural therapy are both viable choices for initial treatment of major depression.Evid Based Ment Health. 2016 Nov;19(4):127. doi: 10.1136/ebmental-2016-102311. Epub 2016 Aug 31. Evid Based Ment Health. 2016. PMID: 27581690 Free PMC article. No abstract available.
References
-
- Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 2003;289:3095-105. - PubMed
-
- Wang PS, Lane M, Olfson M, et al. Twelve-month use of mental health services in the United States: results from the National Comorbidity Survey Replication. Arch Gen Psychiatry 2005;62:629-40. - PubMed
-
- American Psychiatric Association (APA). Practice guideline for the treatment of patients with major depressive disorder. 3rd ed. APA, 2010. - PubMed
-
- Qaseem A, Snow V, Denberg TD, et al. Using second-generation antidepressants to treat depressive disorders: a clinical practice guideline from the American College of Physicians. Ann Intern Med 2008;149:725-33. - PubMed
-
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. National Academies Press, 2001. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources