

Utilization of a Cloud-Based Diabetes Management Program for Insulin Initiation and Titration Enables Collaborative Decision Making Between Healthcare Providers and Patients
- PMID: 26645932
- PMCID: PMC4753582
- DOI: 10.1089/dia.2015.0160
Utilization of a Cloud-Based Diabetes Management Program for Insulin Initiation and Titration Enables Collaborative Decision Making Between Healthcare Providers and Patients
Abstract
Background: Overseeing proper insulin initiation and titration remains a challenging task in diabetes care. Recent advances in mobile technology have enabled new models of collaborative care between patients and healthcare providers (HCPs). We hypothesized that the adoption of such technology could help individuals starting basal insulin achieve better glycemic control compared with standard clinical practice.
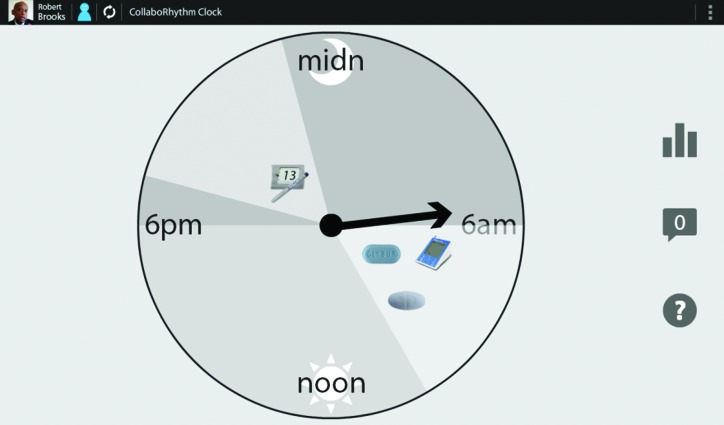
Materials and methods: This was a 12 ± 2-week randomized controlled study with 40 individuals with type 2 diabetes who were starting basal insulin due to poor glycemic control. The control group (n = 20) received standard face-to-face care and phone follow-up as needed in a tertiary center, whereas the intervention group (n = 20) received care through the cloud-based diabetes management program where regular communications about glycemic control and insulin doses were conducted via patient self-tracking tools, shared decision-making interfaces, secure text messages, and virtual visits (audio, video, and shared screen control) instead of office visits.
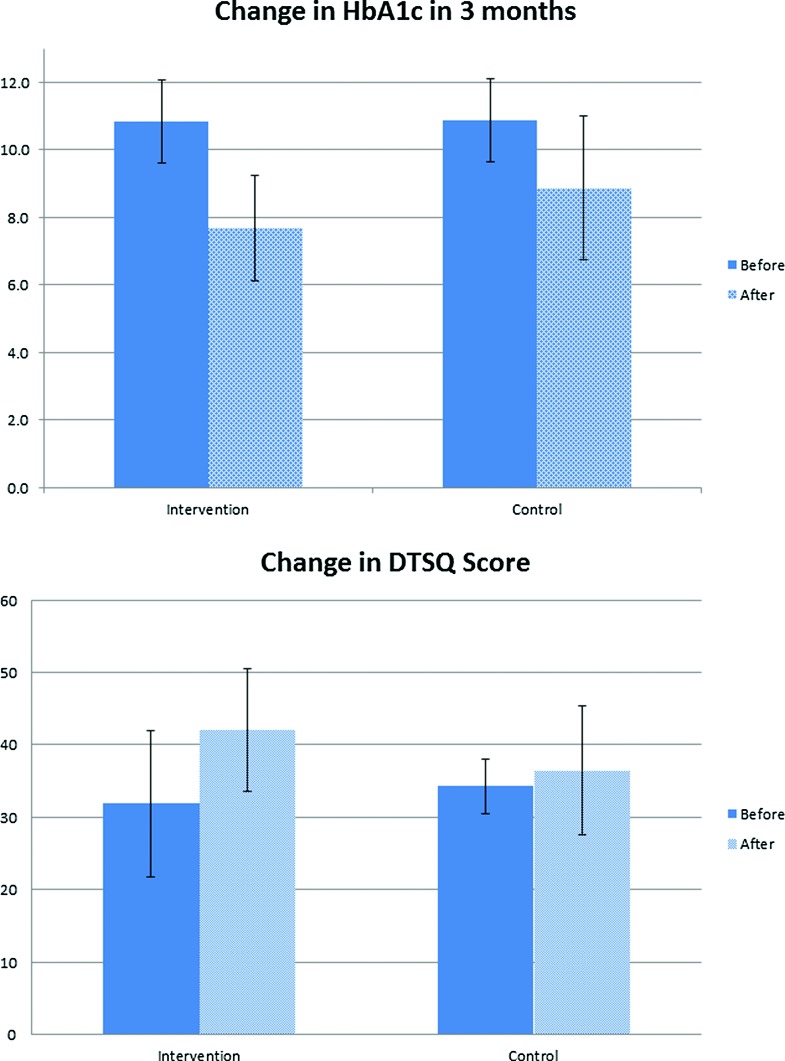
Results: By intention-to-treat analysis, the intervention group achieved a greater hemoglobin A1c decline compared with the control group (3.2 ± 1.5% vs. 2.0% ± 2.0%; P = 0.048). The Diabetes Treatment Satisfaction Questionnaire showed a significant improvement in the intervention group compared with the control group (an increase of 10.1 ± 11.7 vs. 2.1 ± 6.5 points; P = 0.01). HCPs spent less time with patients in the intervention group compared with those in the control group (65.9 min per subject vs. 81.6 min per subject). However, the intervention group required additional training time to use the mobile device.
Conclusions: Mobile health technology could be an effective tool in sharing data, enhancing communication, and improving glycemic control while enabling collaborative decision making in diabetes care.
Figures

Comment in
-
Can Diabetes Management Be Done Effectively Through the Cloud?Diabetes Technol Ther. 2016 Feb;18(2):49-51. doi: 10.1089/dia.2015.0378. Epub 2016 Jan 11. Diabetes Technol Ther. 2016. PMID: 26752348 No abstract available.
References
-
- Peters AL, Legorreta AP, Ossorio RC, et al. : Quality of outpatient care provided to diabetic patients. A health maintenance organization experience. Diabetes Care 1996;19:601–606 - PubMed
-
- World Health Organization: Global Status Report on Noncommunicable Diseases. 2010. www.who.int/nmh/publications/ncd_report_full_en.pdf (accessed February7, 2015) - PubMed
-
- Inzucchi SE, Bergenstal RM, Buse JB, et al. : Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2015;38:140–149 - PubMed
-
- American Diabetes Association: (7) Approaches to glycemic treatment. Diabetes Care 2015;38(Suppl):S41–S48 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical