

Advances in the treatment of newly diagnosed glioblastoma
- PMID: 26646075
- PMCID: PMC4673777
- DOI: 10.1186/s12916-015-0536-8
Advances in the treatment of newly diagnosed glioblastoma
Abstract
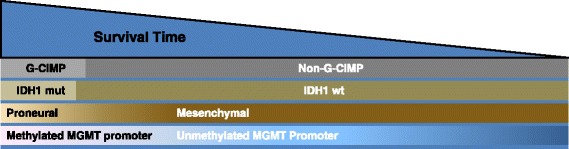
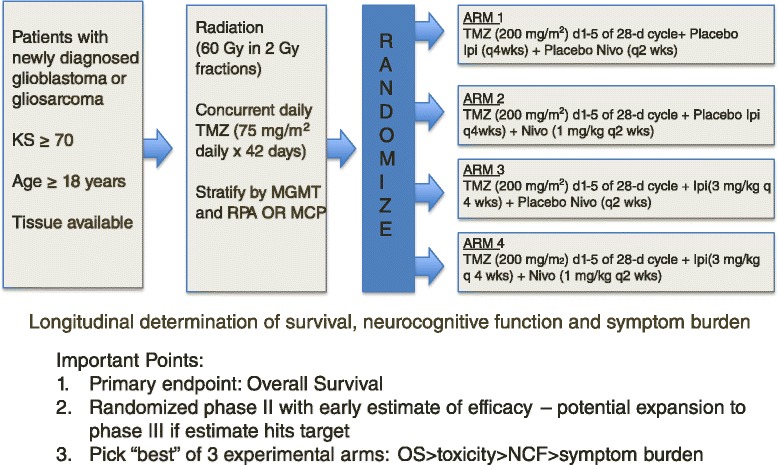
Glioblastoma is a refractory malignancy with limited treatment options at tumor recurrence. Only a small proportion of patients survive 2 years or longer with the current standard of care. Gene expression profiling can segregate newly diagnosed patients into groups with different prognoses, and these biomarkers are being incorporated into a new generation of personalized clinical trials. Using the experience from recently completed large scale, multi-faceted, randomized glioblastoma clinical trials, a new clinical trial paradigm is being established to move promising therapies forward into the newly diagnosed treatment setting. Upcoming trials using the immune check-point inhibitors are an example of this changing paradigm and these and other immunotherapies have potential as promising new treatment modalities for newly diagnosed GB patients.
Figures
Similar articles
-
The Evolving Role of Tumor Treating Fields in Managing Glioblastoma: Guide for Oncologists.Am J Clin Oncol. 2018 Feb;41(2):191-196. doi: 10.1097/COC.0000000000000395. Am J Clin Oncol. 2018. PMID: 28832384 Free PMC article. Review.
-
Management of glioblastoma: State of the art and future directions.CA Cancer J Clin. 2020 Jul;70(4):299-312. doi: 10.3322/caac.21613. Epub 2020 Jun 1. CA Cancer J Clin. 2020. PMID: 32478924 Review.
-
From imaging to biology of glioblastoma: new clinical oncology perspectives to the problem of local recurrence.Clin Transl Oncol. 2018 Aug;20(8):989-1003. doi: 10.1007/s12094-018-1831-6. Epub 2018 Jan 15. Clin Transl Oncol. 2018. PMID: 29335830 Review.
-
Treatment of recurrent glioblastoma: state-of-the-art and future perspectives.Expert Rev Anticancer Ther. 2020 Sep;20(9):785-795. doi: 10.1080/14737140.2020.1807949. Epub 2020 Sep 3. Expert Rev Anticancer Ther. 2020. PMID: 32799576 Review.
-
Glioblastoma multiforme: evidence-based approach to therapy.Expert Rev Anticancer Ther. 2007 Dec;7(12 Suppl):S23-7. doi: 10.1586/14737140.7.12s.S23. Expert Rev Anticancer Ther. 2007. PMID: 18076314 Review.
Cited by
-
Challenges and opportunities in newly diagnosed glioblastoma in the United Kingdom: A Delphi panel.Neurooncol Pract. 2024 Jun 22;11(6):740-752. doi: 10.1093/nop/npae058. eCollection 2024 Dec. Neurooncol Pract. 2024. PMID: 39554782 Free PMC article.
-
Research progress and challenges of the PD-1/PD-L1 axis in gliomas.Cell Biosci. 2024 Sep 27;14(1):123. doi: 10.1186/s13578-024-01305-6. Cell Biosci. 2024. PMID: 39334448 Free PMC article. Review.
-
Unscheduled hospitalization as a potential trigger for specialist palliative care referral in patients with high grade glioma: a retrospective analysis in a tertiary hospital.J Neurooncol. 2025 Jun;173(2):361-368. doi: 10.1007/s11060-025-04993-3. Epub 2025 Mar 6. J Neurooncol. 2025. PMID: 40048038
-
Frontiers in Anti-Cancer Drug Discovery: Challenges and Perspectives of Metformin as Anti-Angiogenic Add-On Therapy in Glioblastoma.Cancers (Basel). 2021 Dec 27;14(1):112. doi: 10.3390/cancers14010112. Cancers (Basel). 2021. PMID: 35008275 Free PMC article. Review.
-
Glioblastoma: new therapeutic strategies to address cellular and genomic complexity.Oncotarget. 2017 Dec 20;9(10):9540-9554. doi: 10.18632/oncotarget.23476. eCollection 2018 Feb 6. Oncotarget. 2017. PMID: 29507709 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
