

Handoffs in the Intensive Care Unit
- PMID: 26646283
- PMCID: PMC5898635
- DOI: 10.1177/1062860615617238
Handoffs in the Intensive Care Unit
Abstract
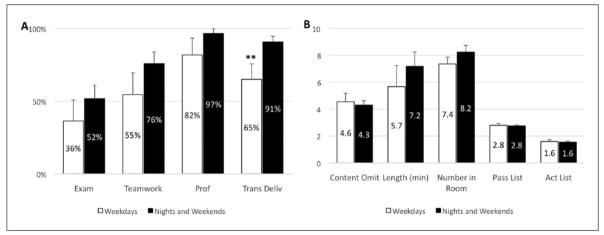
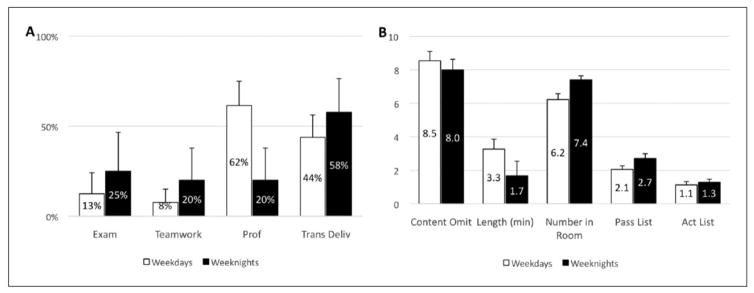
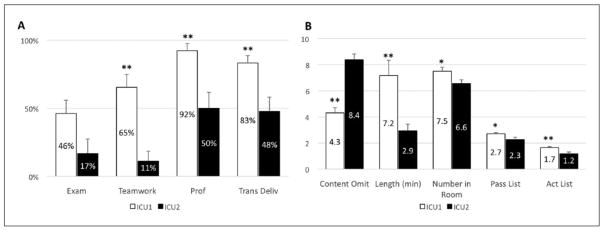
Operating room (OR) to intensive care unit (ICU) handoffs are complex and known to be associated with adverse events and patient harm. The authors hypothesized that handoff quality diminishes during nights/weekends and that bedside handoff practices are similar between ICUs of the same health system. Bedside OR-to-ICU handoffs were directly observed in 2 surgical ICUs with different patient volumes. Handoff quality measures were compared within the ICUs on weekdays versus nights/weekends as well as between the high- and moderate-volume ICUs. In the high-volume ICU, transmitter delivery scores were significantly better during off hours, while other measures were not different. High-volume ICU scores were consistently better than those in the moderate-volume ICU. Bedside handoff practices are not worse during off hours and may be better in ICUs used to a higher patient volume. Specific handoff protocols merit evaluation and training to ensure consistent practices in different ICU models and at different times.
Keywords: handoff; sign-out; transition in care; weekend effect.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Date DF, Sanfey H, Mellinger J, Dunnington G. Handoffs in general surgery residency, an observation of intern and senior residents. Am J Surg. 2013;206:693–697. - PubMed
-
- Nagpal K, Abboudi M, Manchanda C, et al. Improving postoperative handover: a prospective observational study. Am J Surg. 2013;206:494–501. - PubMed
-
- The Joint Commission. [Accessed October 22, 2015];Sentinel event data: root causes by event type 2004-2Q. 2015 http://www.jointcommission.org/assets/1/18/Root_Causes_Event_Type_2004-2....
-
- Gawande AA, Zinner MJ, Studdert DM, Brennan TA. Analysis of errors reported by surgeons at three teaching hospitals. Surgery. 2003;133:614–621. - PubMed
-
- Singh H, Thomas EJ, Petersen LA, Studdert DM. Medical errors involving trainees: a study of closed malpractice claims from 5 insurers. Arch Intern Med. 2007;167:2030–2036. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
