

Among Unstable Angina and Non-ST-Elevation Myocardial Infarction Patients, Transient Myocardial Ischemia and Early Invasive Treatment Are Predictors of Major In-hospital Complications
- PMID: 26646595
- PMCID: PMC4896865
- DOI: 10.1097/JCN.0000000000000310
Among Unstable Angina and Non-ST-Elevation Myocardial Infarction Patients, Transient Myocardial Ischemia and Early Invasive Treatment Are Predictors of Major In-hospital Complications
Abstract
Background: Treatment for unstable angina (UA) or non-ST-elevation myocardial infarction (NSTEMI) is aimed at plaque stabilization to prevent infarction. Two treatment strategies are (1) invasive (ie, cardiac catheterization laboratory <24 hours after admission) or (2) selectively invasive (ie, medications with cardiac catheterization laboratory >24 hours for recurrent symptoms). However, it is not known if the frequency of transient myocardial ischemia (TMI) or complications during hospitalization varies by treatment.
Purpose: We aimed to (1) examine occurrence of TMI in UA/NSTEMI, (2) compare frequency of TMI by treatment pathway, and (3) determine predictors of in-hospital complications (ie, death, myocardial infarction [MI], pulmonary edema, shock, dysrhythmia with intervention).
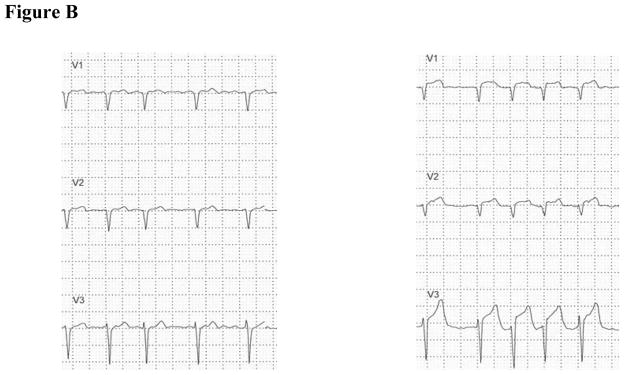
Methods: Hospitalized patients with coronary artery disease (ie, history of MI, percutaneous coronary intervention/stent, coronary artery bypass graft, >50% lesion via angiogram, or positive troponin) were recruited, and 12-lead electrocardiogram Holter initiated. Clinicians, blinded to Holter data, decided treatment strategy; offline analysis was done after discharge. Transient myocardial ischemia was defined as more than 1-mm ST segment ↑ or ↓, in more than 1 electrocardiographic lead, more than 1 minute.
Results: Of 291 patients, 91% were white, 66% were male, 44% had prior MI, and 59% had prior percutaneous coronary intervention/stent or coronary artery bypass graft. Treatment pathway was early in 123 (42%) and selective in 168 (58%). Forty-nine (17%) had TMI: 19 (15%) early invasive, 30 (18%) selective (P = .637). Acute MI after admission was higher in patients with TMI regardless of treatment strategy (early: no TMI 4% vs yes TMI 21%; P = .020; selective: no TMI 1% vs yes TMI 13%; P = .0004). Predictors of major in-hospital complication were TMI (odds ratio, 9.9; 95% confidence interval, 3.84-25.78) and early invasive treatment (odds ratio 3.5; 95% confidence interval, 1.23-10.20).
Conclusions: In UA/NSTEMI patients treated with contemporary therapies, TMI is not uncommon. The presence of TMI and early invasive treatment are predictors of major in-hospital complications.
Conflict of interest statement
Conflicts of interest: none
Figures

References
-
- Khera S, Kolte D, Aronow WS, Palaniswamy C, Subramanian KS, Hashim T, Mujib M, Jain D, Paudel R, Ahmed A, Frishman WH, Bhatt DL, Panza JA, Fonarow GC. Non-ST-elevation myocardial infarction in the United States: contemporary trends in incidence, utilization of the early invasive strategy, and in-hospital outcomes. J Am Heart Assoc. 2014;3(4) - PMC - PubMed
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Judd SE, Kissela BM, Lackland DT, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Matchar DB, McGuire DK, Mohler ER, 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Willey JZ, Woo D, Yeh RW, Turner MB C. American Heart Association Statistics, and S. Stroke Statistics. Heart disease and stroke statistics--2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29–322. - PubMed
-
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Jr, Ganiats TG, Holmes DR, Jr, Jaffe AS, Jneid H, Kelly RF, Kontos MC, Levine GN, Liebson PR, Mukherjee D, Peterson ED, Sabatine MS, Smalling RW, Zieman SJ. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64(24):e139–228. - PubMed
-
- Cannon CP, Weintraub WS, Demopoulos LA, Vicari R, Frey MJ, Lakkis N, Neumann FJ, Robertson DH, DeLucca PT, DiBattiste PM, Gibson CM, Braunwald E. Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med. 2001;344(25):1879–87. - PubMed
-
- Fox KA, Clayton TC, Damman P, Pocock SJ, de Winter RJ, Tijssen JG, Lagerqvist B, Wallentin L, Collaboration FIR. Long-term outcome of a routine versus selective invasive strategy in patients with non-ST-segment elevation acute coronary syndrome a meta-analysis of individual patient data. J Am Coll Cardiol. 2010;55(22):2435–45. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
