

Afatinib beyond progression in patients with non-small-cell lung cancer following chemotherapy, erlotinib/gefitinib and afatinib: phase III randomized LUX-Lung 5 trial
- PMID: 26646759
- PMCID: PMC4769992
- DOI: 10.1093/annonc/mdv597
Afatinib beyond progression in patients with non-small-cell lung cancer following chemotherapy, erlotinib/gefitinib and afatinib: phase III randomized LUX-Lung 5 trial
Abstract
Background: Afatinib has demonstrated clinical benefit in patients with non-small-cell lung cancer progressing after treatment with erlotinib/gefitinib. This phase III trial prospectively assessed whether continued irreversible ErbB-family blockade with afatinib plus paclitaxel has superior outcomes versus switching to chemotherapy alone in patients acquiring resistance to erlotinib/gefitinib and afatinib monotherapy.
Patients and methods: Patients with relapsed/refractory disease following ≥1 line of chemotherapy, and whose tumors had progressed following initial disease control (≥12 weeks) with erlotinib/gefitinib and thereafter afatinib (50 mg/day), were randomized 2:1 to receive afatinib plus paclitaxel (40 mg/day; 80 mg/m(2)/week) or investigator's choice of single-agent chemotherapy. The primary end point was progression-free survival (PFS). Other end points included objective response rate (ORR), overall survival (OS), safety and patient-reported outcomes.
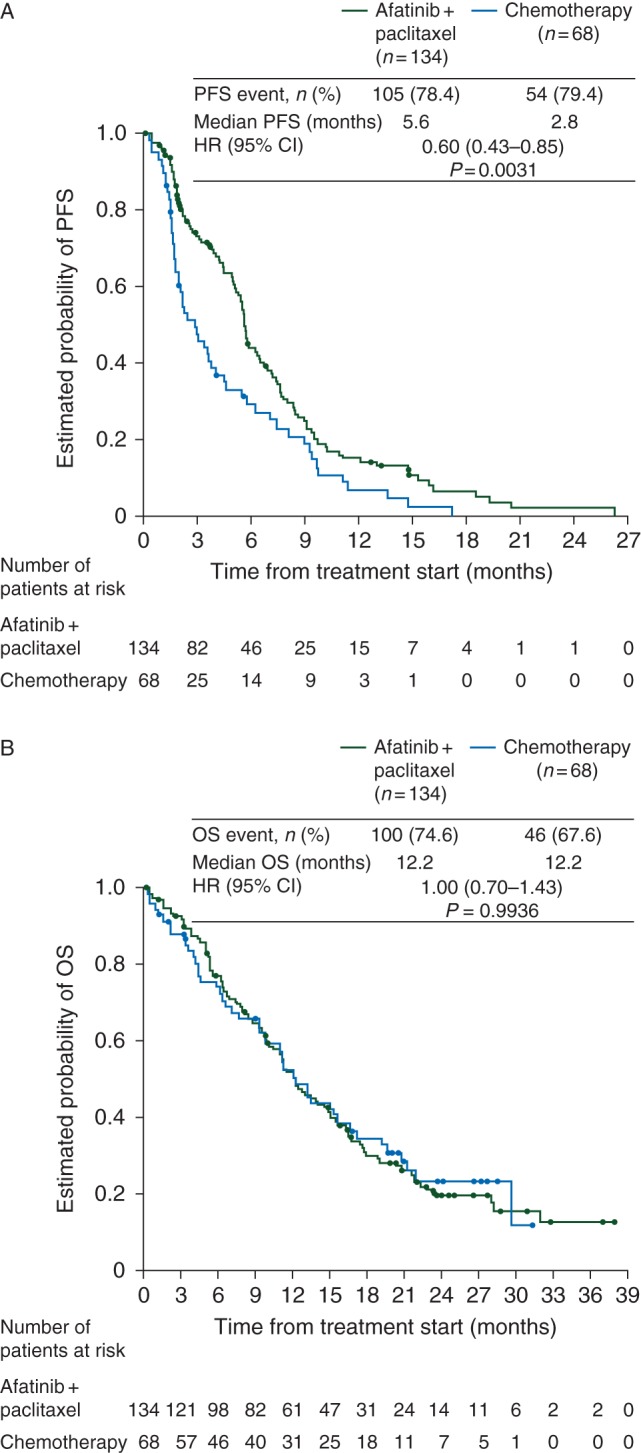
Results: Two hundred and two patients with progressive disease following clinical benefit from afatinib were randomized to afatinib plus paclitaxel (n = 134) or single-agent chemotherapy (n = 68). PFS (median 5.6 versus 2.8 months, hazard ratio 0.60, P = 0.003) and ORR (32.1% versus 13.2%, P = 0.005) significantly improved with afatinib plus paclitaxel. There was no difference in OS. Global health status/quality of life was maintained with afatinib plus paclitaxel over the entire treatment period. The median treatment duration was 133 and 51 days with afatinib plus paclitaxel and single-agent chemotherapy, respectively; 48.5% of patients receiving afatinib plus paclitaxel and 30.0% of patients receiving single-agent chemotherapy experienced drug-related grade 3/4 adverse events. Treatment-related adverse events were consistent with those previously reported with each agent.
Conclusion: Afatinib plus paclitaxel improved PFS and ORR compared with single-agent chemotherapy in patients who acquired resistance to erlotinib/gefitinib and progressed on afatinib after initial benefit. LUX-Lung 5 is the first prospective trial to demonstrate the benefit of continued ErbB targeting post-progression, versus switching to single-agent chemotherapy.
Trial registration number: NCT01085136 (clinicaltrials.gov).
Keywords: NSCLC; afatinib; paclitaxel; squamous cell.
© The Author 2015. Published by Oxford University Press on behalf of the European Society for Medical Oncology.
Figures
Comment in
-
Being molecular in the molecular age.Ann Oncol. 2016 Mar;27(3):367-8. doi: 10.1093/annonc/mdw002. Ann Oncol. 2016. PMID: 26924595 No abstract available.
-
What is the clinical impact of the LUX-Lung 5 trial?Ann Oncol. 2016 Jun;27(6):1171-1172. doi: 10.1093/annonc/mdw102. Epub 2016 Mar 2. Ann Oncol. 2016. PMID: 26940690 No abstract available.
-
Reply to the letter to the editor 'What is the clinical impact of the LUX-Lung 5 trial?' by Addeo.Ann Oncol. 2016 Jun;27(6):1172-1173. doi: 10.1093/annonc/mdw144. Epub 2016 Mar 30. Ann Oncol. 2016. PMID: 27029703 No abstract available.
-
Afatinib plus chemotherapy versus chemotherapy alone after progression on afatinib: new insights on old question?Ann Transl Med. 2016 Oct;4(Suppl 1):S31. doi: 10.21037/atm.2016.09.45. Ann Transl Med. 2016. PMID: 27867999 Free PMC article. No abstract available.
References
-
- Lee CK, Brown C, Gralla RJ et al. . Impact of EGFR inhibitor in non-small cell lung cancer on progression-free and overall survival: a meta-analysis. J Natl Cancer Inst 2013; 105: 595–605. - PubMed
-
- Riely GJ, Kris MG, Zhao B et al. . Prospective assessment of discontinuation and reinitiation of erlotinib or gefitinib in patients with acquired resistance to erlotinib or gefitinib followed by the addition of everolimus. Clin Cancer Res 2007; 13: 5150–5155. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
