

A Randomized Study Comparing Parathyroidectomy with Cinacalcet for Treating Hypercalcemia in Kidney Allograft Recipients with Hyperparathyroidism
- PMID: 26647424
- PMCID: PMC4978046
- DOI: 10.1681/ASN.2015060622
A Randomized Study Comparing Parathyroidectomy with Cinacalcet for Treating Hypercalcemia in Kidney Allograft Recipients with Hyperparathyroidism
Abstract
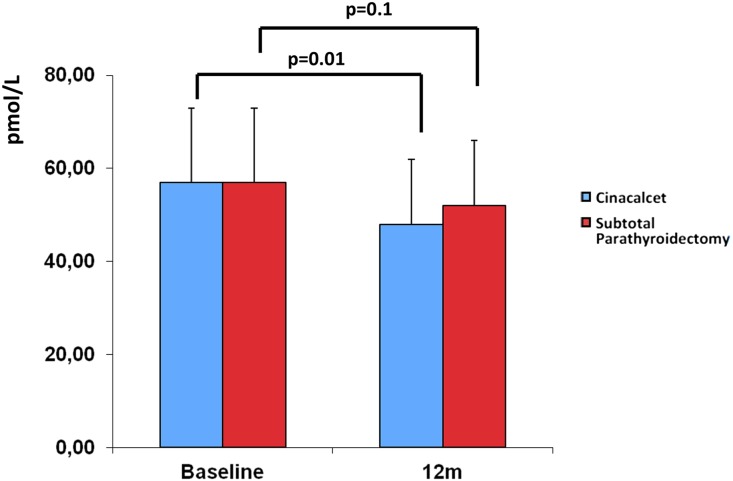
Tertiary hyperparathyroidism is a common cause of hypercalcemia after kidney transplant. We designed this 12-month, prospective, multicenter, open-label, randomized study to evaluate whether subtotal parathyroidectomy is more effective than cinacalcet for controlling hypercalcemia caused by persistent hyperparathyroidism after kidney transplant. Kidney allograft recipients with hypercalcemia and elevated intact parathyroid hormone (iPTH) concentration were eligible if they had received a transplant ≥6 months before the study and had an eGFR>30 ml/min per 1.73 m(2) The primary end point was the proportion of patients with normocalcemia at 12 months. Secondary end points were serum iPTH concentration, serum phosphate concentration, bone mineral density, vascular calcification, renal function, patient and graft survival, and economic cost. In total, 30 patients were randomized to receive cinacalcet (n=15) or subtotal parathyroidectomy (n=15). At 12 months, ten of 15 patients in the cinacalcet group and 15 of 15 patients in the parathyroidectomy group (P=0.04) achieved normocalcemia. Normalization of serum phosphate concentration occurred in almost all patients. Subtotal parathyroidectomy induced greater reduction of iPTH and associated with a significant increase in femoral neck bone mineral density; vascular calcification remained unchanged in both groups. The most frequent adverse events were digestive intolerance in the cinacalcet group and hypocalcemia in the parathyroidectomy group. Surgery would be more cost effective than cinacalcet if cinacalcet duration reached 14 months. All patients were alive with a functioning graft at the end of follow-up. In conclusion, subtotal parathyroidectomy was superior to cinacalcet in controlling hypercalcemia in these patients with kidney transplants and persistent hyperparathyroidism.
Keywords: calcium; hyperparathyroidism; renal transplantation.
Copyright © 2016 by the American Society of Nephrology.
Figures


Comment in
-
Parathyroidectomy or Calcimimetic to Treat Hypercalcemia after Kidney Transplantation?J Am Soc Nephrol. 2016 Aug;27(8):2221-4. doi: 10.1681/ASN.2015121349. Epub 2016 Jan 15. J Am Soc Nephrol. 2016. PMID: 26772195 Free PMC article. No abstract available.
References
-
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, Held PJ, Port FK: Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med 341: 1725–1730, 1999 - PubMed
-
- Morris PJ: Transplantation--a medical miracle of the 20th century. N Engl J Med 351: 2678–2680, 2004 - PubMed
-
- Gondos A, Döhler B, Brenner H, Opelz G: Kidney graft survival in Europe and the United States: Strikingly different long-term outcomes. Transplantation 95: 267–274, 2013 - PubMed
-
- Schwarz A, Mengel M, Gwinner W, Radermacher J, Hiss M, Kreipe H, Haller H: Risk factors for chronic allograft nephropathy after renal transplantation: A protocol biopsy study. Kidney Int 67: 341–348, 2005 - PubMed
-
- Pihlstrøm H, Dahle DO, Mjøen G, Pilz S, März W, Abedini S, Holme I, Fellström B, Jardine AG, Holdaas H: Increased risk of all-cause mortality and renal graft loss in stable renal transplant recipients with hyperparathyroidism. Transplantation 99: 351–359, 2015 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
