

Arthroscopic-Assisted Combined Dorsal and Volar Scapholunate Ligament Reconstruction with Tendon Graft for Chronic SL Instability
- PMID: 26649257
- PMCID: PMC4626228
- DOI: 10.1055/s-0035-1565927
Arthroscopic-Assisted Combined Dorsal and Volar Scapholunate Ligament Reconstruction with Tendon Graft for Chronic SL Instability
Abstract
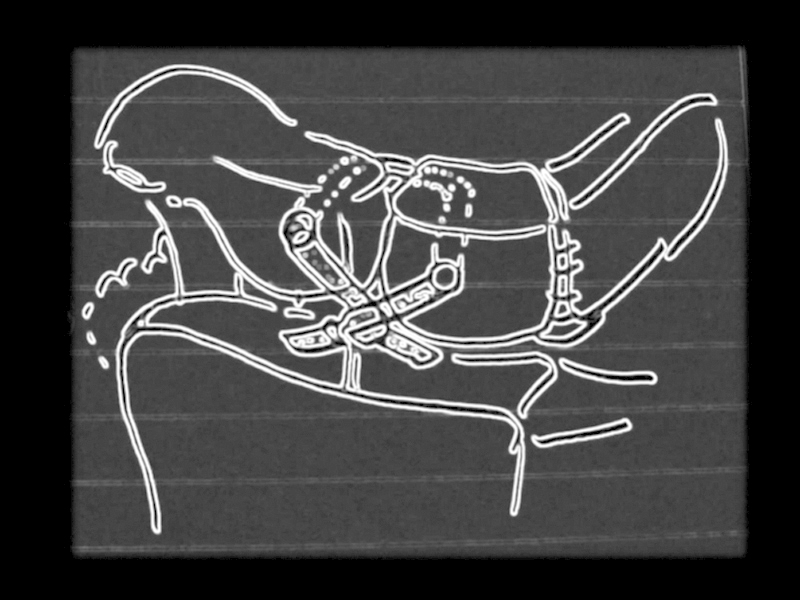
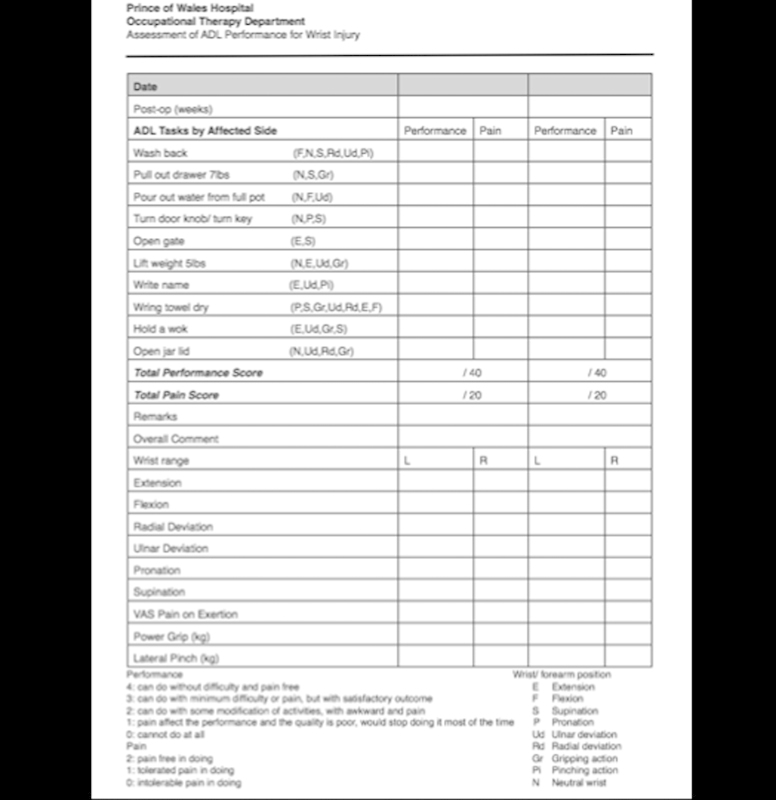
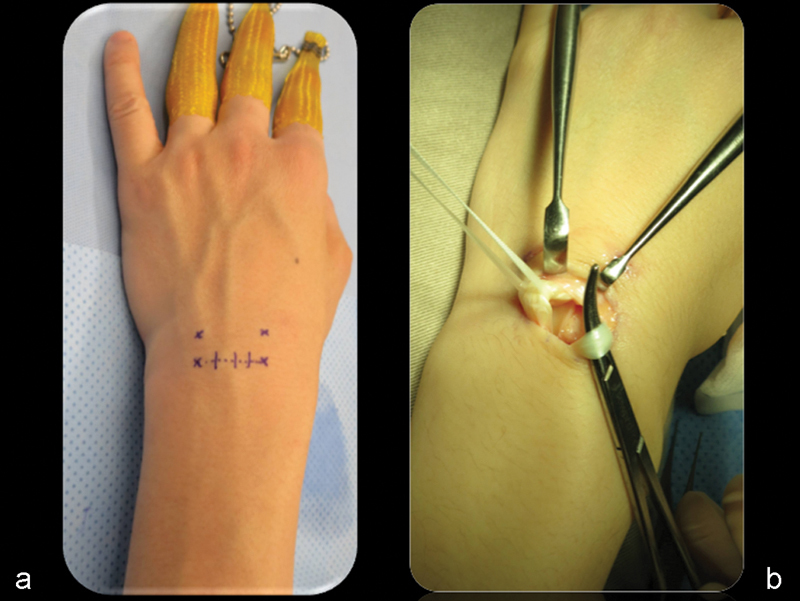
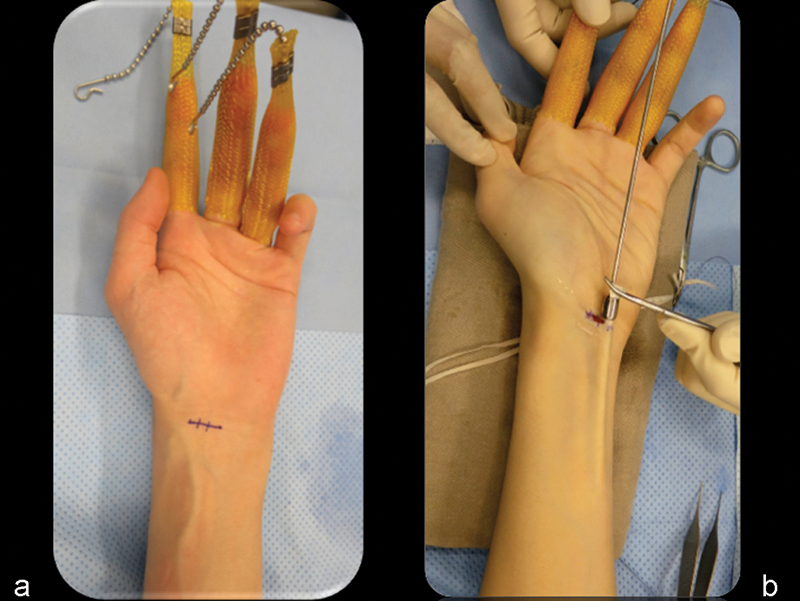
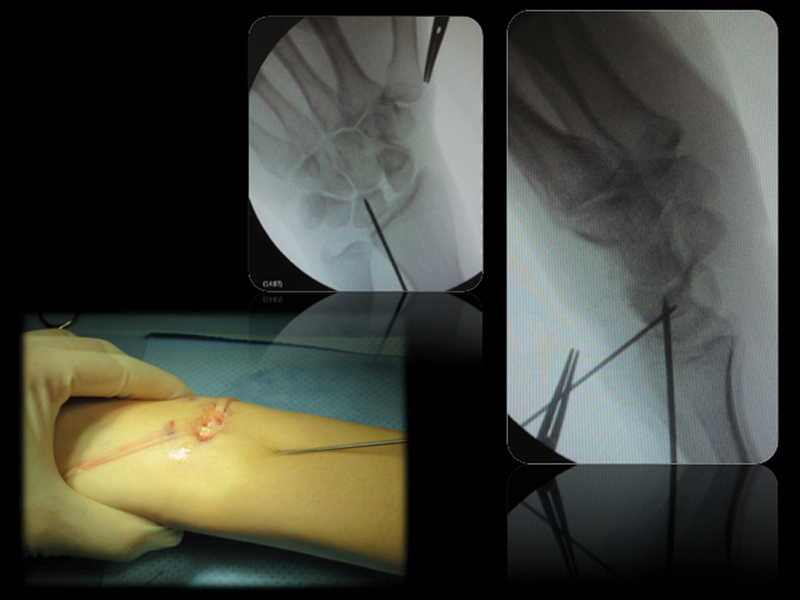
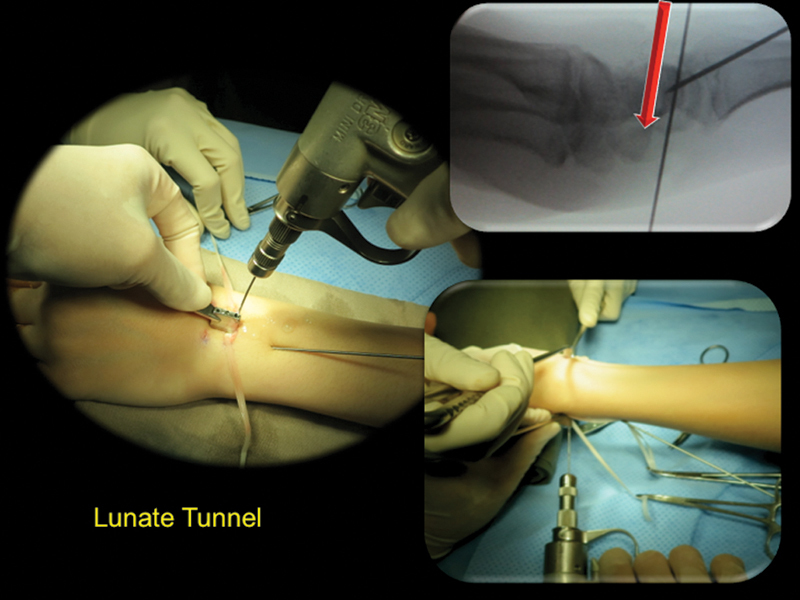
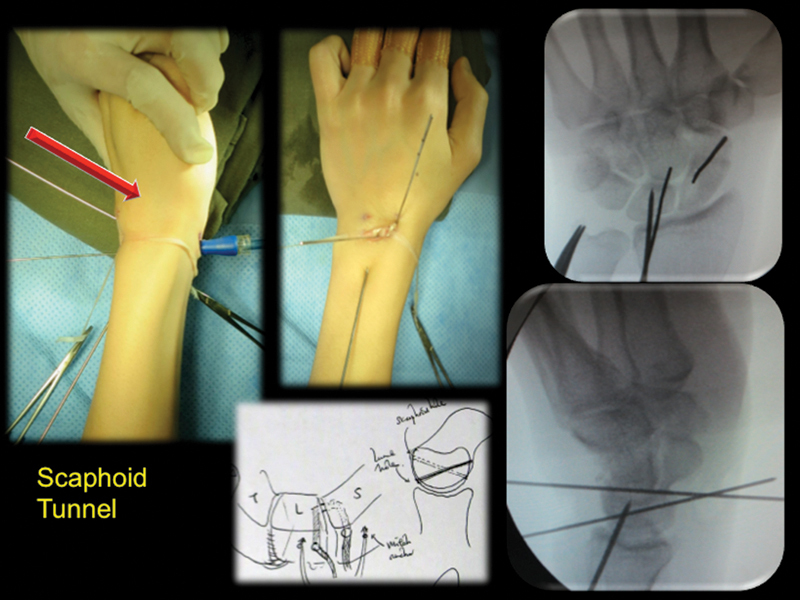
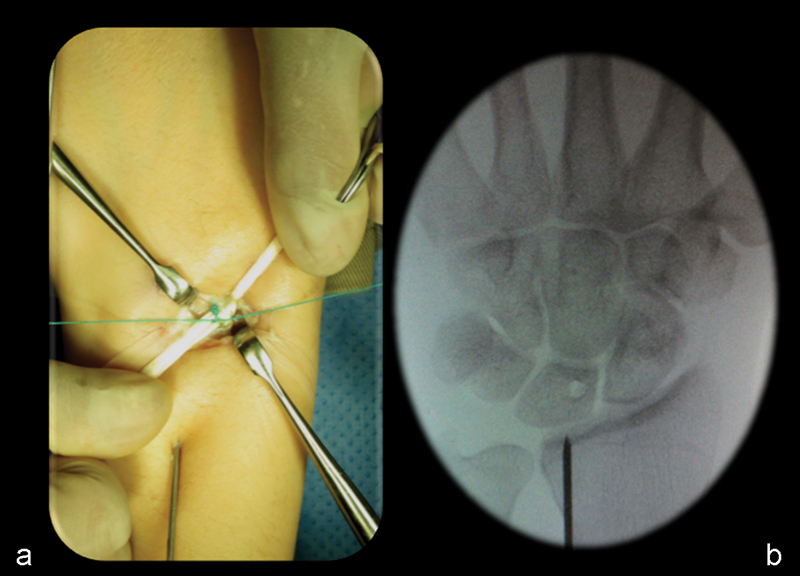
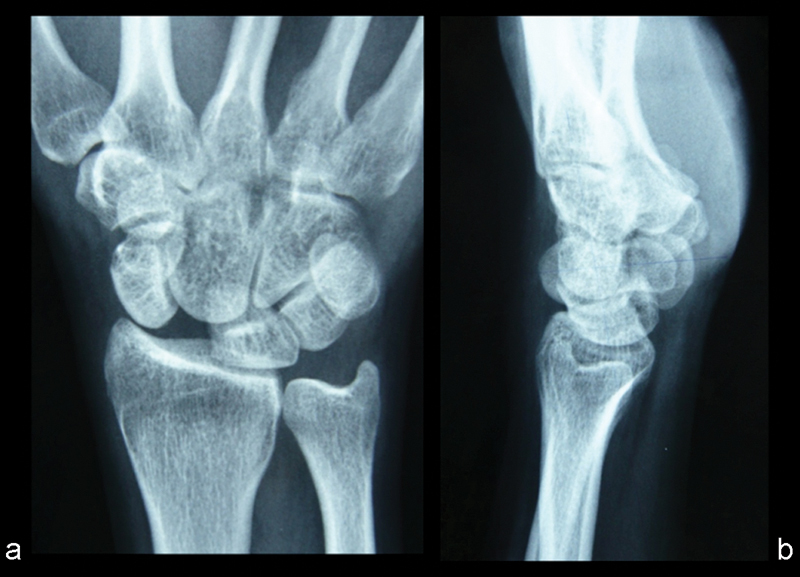
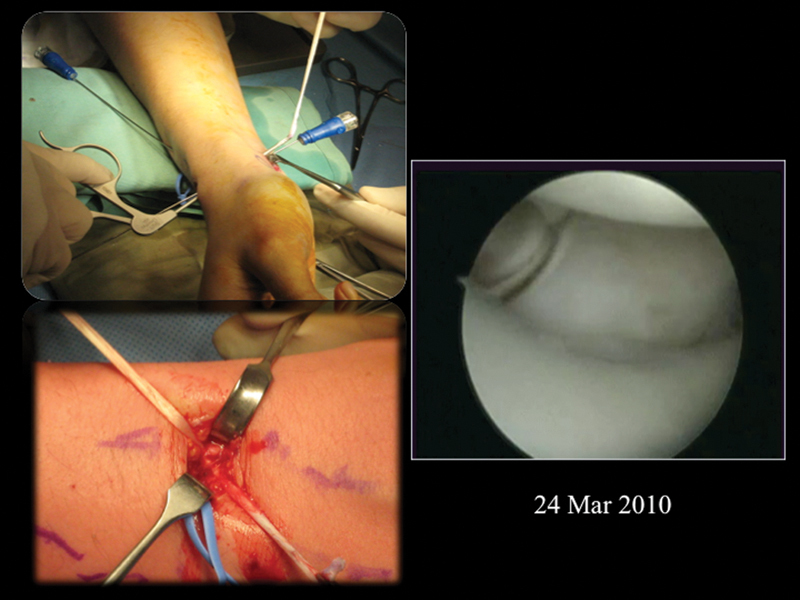
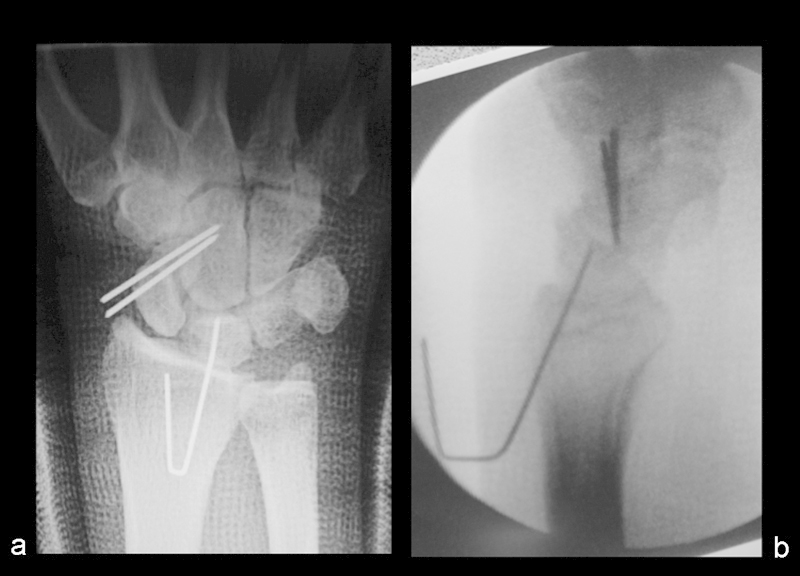
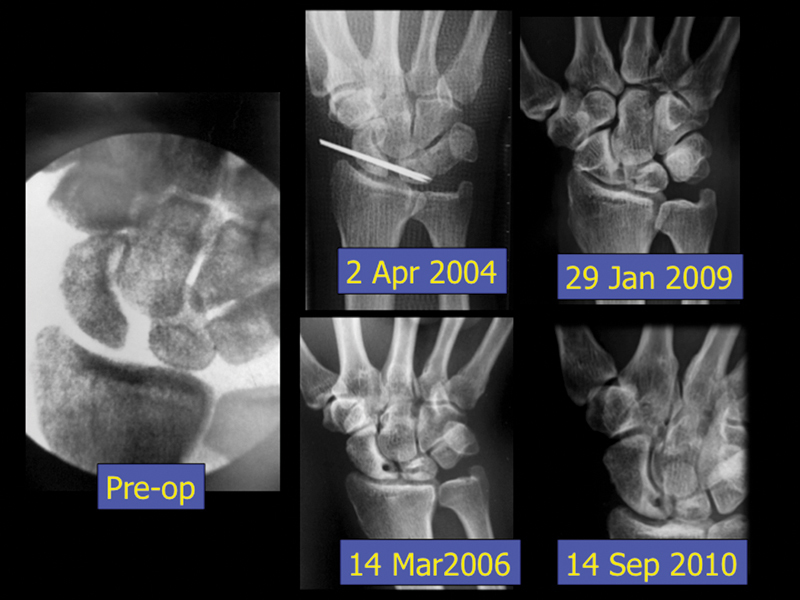
Background Both the dorsal and the volar portion of the scapholunate interosseous ligament (SLIL) are major stabilizers of the scapholunate (SL) joint. Most reconstruction methods to restore SL stability do not address the volar constraints and frequently fail to reduce the SL gapping. Wrist arthroscopy allows a complete evaluation of the SL interval, accompanying ligament status, and associated SL advanced collapse (SLAC) wrist changes. It enables simultaneous reconstruction of the dorsal and palmar SL ligaments anatomically with the use tendon graft in a boxlike structure. Materials and Methods From October 2002 to June 2012, the treatment method was applied in 17 patients of chronic SL instability of average duration of 9.5 months (range 1.5-18 months). There were three Geissler grade 3 and 14 grade 4 instability cases. The average preoperative SL interval was 4.9 mm (range 3-9 mm). Dorsal intercalated segment instability (DISI) deformity was present in 13 patients. Six patients had stage 1 SLAC wrist change radiologically. Concomitant procedures were performed in four patients. Description of Technique With the assistance of arthroscopy and intraoperative imaging as a guide, a combined limited dorsal and volar incision exposed the dorsal and palmar SL interval without violating the wrist joint capsule. Bone tunnels of 2.4 mm were made on the proximal scaphoid and lunate. A palmaris longus tendon graft was delivered through the wrist capsule and the bone tunnels to reduce and connect the two bones in a boxlike fashion. Once the joint diastasis is reduced and any DISI malrotation corrected, the tendon graft was knotted and sutured on the dorsal surface of the SL joint extra-capsularly in a shoe-lacing manner. The scaphocapitate joint was transfixed with Kirschner wires (K-wires) to protect the reconstruction for 6-8 weeks. Results The average follow-up was 48.3 months (range 11-132 months). Thirteen returned to their preinjury job level. Eleven patients had no wrist pain, and six had some pain on either maximum exertion or at the extreme of motion. The average total pain score was 1.7/20 compared with the preoperative score of 8.3/20. The postoperative average total wrist performance score was 37.8/40, with an improvement of 35%. The average extension range improved for 13%, flexion range 16%, radial deviation 13%, and ulnar deviation 27%. Mean grip strength was 32.8 kg (120% of the preoperative status, 84% of the contralateral side). The average SL interval was 2.9 mm (range 1.6-5.5 mm). Recurrence of a DISI deformity was noted in four patients without symptoms. Ischemic change of proximal scaphoid was noted in one case without symptoms or progression. There were no major complications. All patients were satisfied with the procedure and outcome. Conclusion Our method of reconstructing both the dorsal and volar SL ligament, in a minimally invasive way, is a logical and effective technique to improve SL stability. The potential risk of ischemic necrosis of the carpal bone is minimized by preservation of the scaphoid blood supply, the small size of the bone tunnels created, and the inclusion of the capsule at the reconstruction site.
Keywords: SL dissociation; scapholunate ligament; tendon graft; wrist arthroscopy; wrist surgery.
Conflict of interest statement
Figures




Similar articles
-
Perilunate Dislocations: Reduction and Stabilization.JBJS Essent Surg Tech. 2023 Nov 29;13(4):e23.00031. doi: 10.2106/JBJS.ST.23.00031. eCollection 2023 Oct-Dec. JBJS Essent Surg Tech. 2023. PMID: 38357468 Free PMC article.
-
Dorsal capsulodesis associated with arthoscopy-assisted scapholunate ligament reconstruction using a palmaris longus tendon graft.Rev Bras Ortop. 2017 Oct 28;52(6):676-684. doi: 10.1016/j.rboe.2016.11.010. eCollection 2017 Nov-Dec. Rev Bras Ortop. 2017. PMID: 29234651 Free PMC article.
-
Dorsal Scapholunate Ligament Complex Reconstruction Using Suture Tape-Augmented Autologous Free Tendon Graft for Chronic Scapholunate Dissociation.Clin Orthop Surg. 2024 Oct;16(5):790-799. doi: 10.4055/cios24032. Epub 2024 Jun 4. Clin Orthop Surg. 2024. PMID: 39364099 Free PMC article.
-
Treatment of chronic scapholunate dissociation with tenodesis: A systematic review.Hand Surg Rehabil. 2018 Apr;37(2):65-76. doi: 10.1016/j.hansur.2017.12.001. Epub 2017 Dec 29. Hand Surg Rehabil. 2018. PMID: 29292109
-
Arthroscopic-Assisted Volar Scapholunate Capsulodesis: A New Technique.J Hand Surg Am. 2022 Nov;47(11):1124.e1-1124.e6. doi: 10.1016/j.jhsa.2022.05.018. Epub 2022 Aug 12. J Hand Surg Am. 2022. PMID: 35965143 Review.
Cited by
-
Scapholunate Ligament Internal Brace 360-Degree Tenodesis (SLITT) Procedure.J Wrist Surg. 2018 Sep;7(4):336-340. doi: 10.1055/s-0038-1625954. Epub 2018 Jan 30. J Wrist Surg. 2018. PMID: 30174992 Free PMC article.
-
Radiologic Evolution after Scapholunate Dorsal Capsulodesis for Chronic Tears.J Wrist Surg. 2023 Feb 28;12(5):433-438. doi: 10.1055/s-0043-1764159. eCollection 2023 Oct. J Wrist Surg. 2023. PMID: 37841361 Free PMC article.
-
Cadaveric Testing of a Novel Scapholunate Ligament Reconstruction.J Wrist Surg. 2018 Apr;7(2):141-147. doi: 10.1055/s-0037-1607326. Epub 2017 Oct 26. J Wrist Surg. 2018. PMID: 29576920 Free PMC article.
-
Scapholunate Ligament Injuries.J Hand Surg Glob Online. 2024 Apr 1;6(3):245-267. doi: 10.1016/j.jhsg.2024.01.015. eCollection 2024 May. J Hand Surg Glob Online. 2024. PMID: 38817761 Free PMC article. Review.
-
The Current Role of Arthroscopy in Traumatic Wrist Injuries: An Expert Survey.J Wrist Surg. 2022 Aug 1;12(3):192-198. doi: 10.1055/s-0042-1750875. eCollection 2023 Jun. J Wrist Surg. 2022. PMID: 37223380 Free PMC article.
References
-
- Daniels J M II, Zook E G, Lynch J M. Hand and wrist injuries: Part I. Nonemergent evaluation. Am Fam Physician. 2004;69(8):1941–1948. - PubMed
-
- Moran S L, Ford K S, Wulf C A, Cooney W P. Outcomes of dorsal capsulodesis and tenodesis for treatment of scapholunate instability. J Hand Surg Am. 2006;31(9):1438–1446. - PubMed
-
- Linscheid R L, Dobyns J H. Treatment of scapholunate dissociation. Rotatory subluxation of the scaphoid. Hand Clin. 1992;8(4):645–652. - PubMed
-
- Almquist E E, Bach A W, Sack J T, Fuhs S E, Newman D M. Four-bone ligament reconstruction for treatment of chronic complete scapholunate separation. J Hand Surg Am. 1991;16(2):322–327. - PubMed
-
- Brunelli G A, Brunelli G R. A new technique to correct carpal instability with scaphoid rotary subluxation: a preliminary report. J Hand Surg Am. 1995;20(3 Pt 2):S82–S85. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
