

Impaired Immune Response in Elderly Burn Patients: New Insights Into the Immune-senescence Phenotype
- PMID: 26649579
- PMCID: PMC4899096
- DOI: 10.1097/SLA.0000000000001408
Impaired Immune Response in Elderly Burn Patients: New Insights Into the Immune-senescence Phenotype
Abstract
Objective: Comparing the inflammatory and immunological trajectories in burned adults versus burned elderly patients to gain novel insights and better understanding why elderly have poor outcomes.
Summary background data: Despite receiving the same treatment and clinical consideration as all other burn patients, elderly patients continue to have substantially poorer outcomes compared with adults. In light of an aging population, gaining a better understanding of their susceptibility to complications and creating new treatment strategies is imperative.
Methods: We included 130 burn patients (94 adults: <65 years old and 36 elderly: ≥65 years old) and 10 healthy controls in this study. Immune activity and expression was assessed using bioplex at various time points. Clinical outcomes such as infection, sepsis, and mortality were prospectively collected.
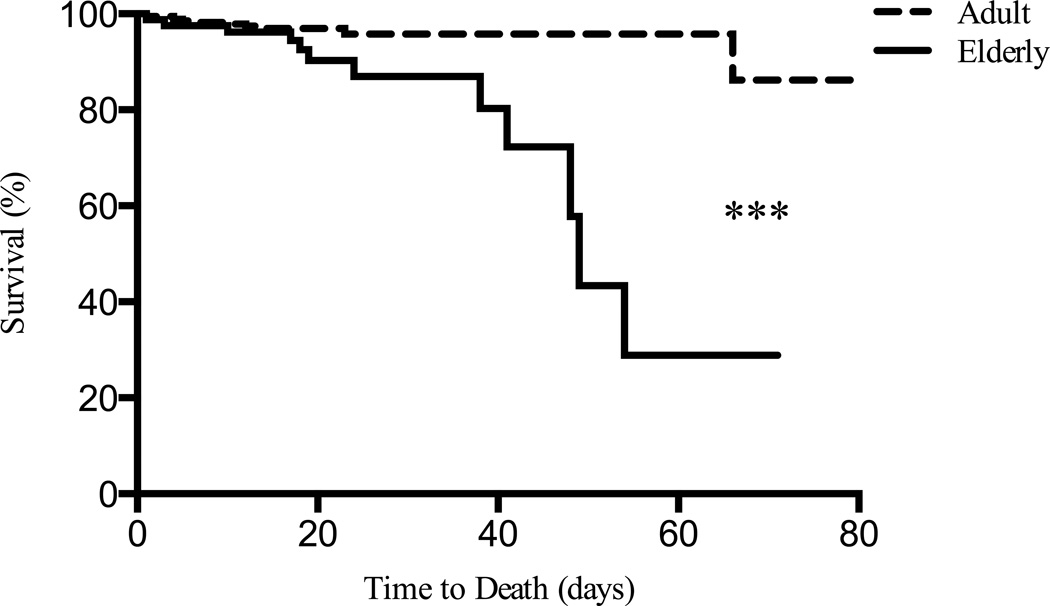
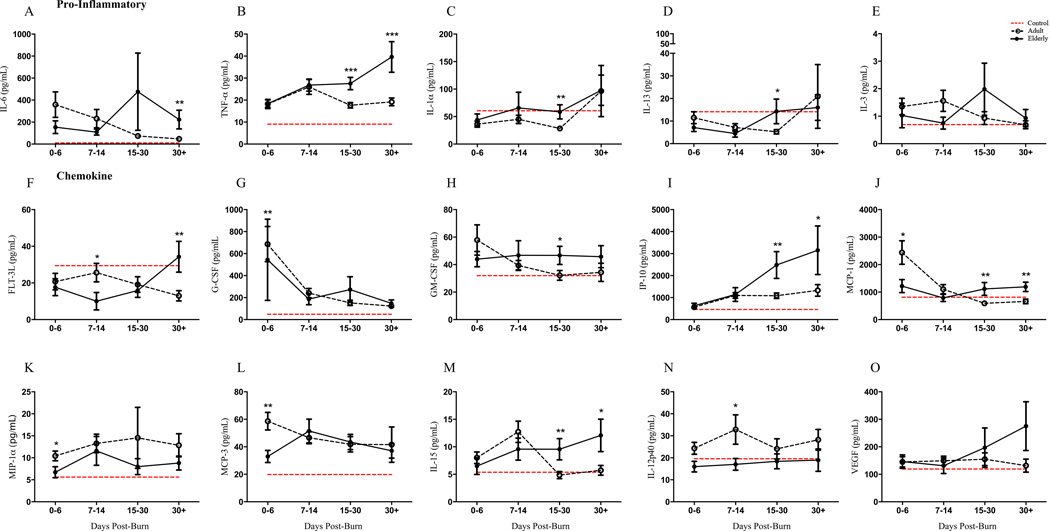
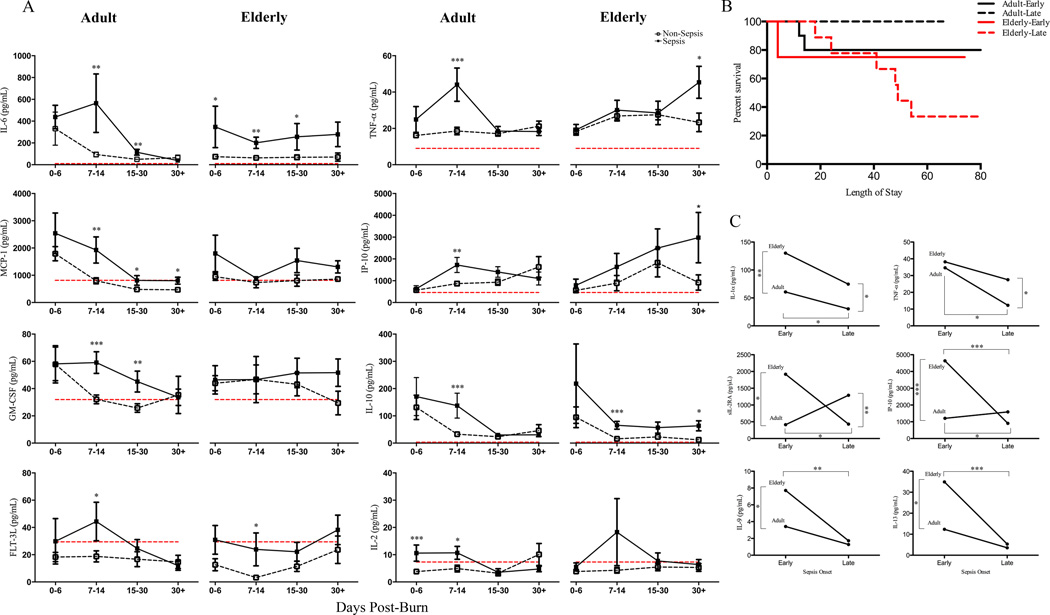
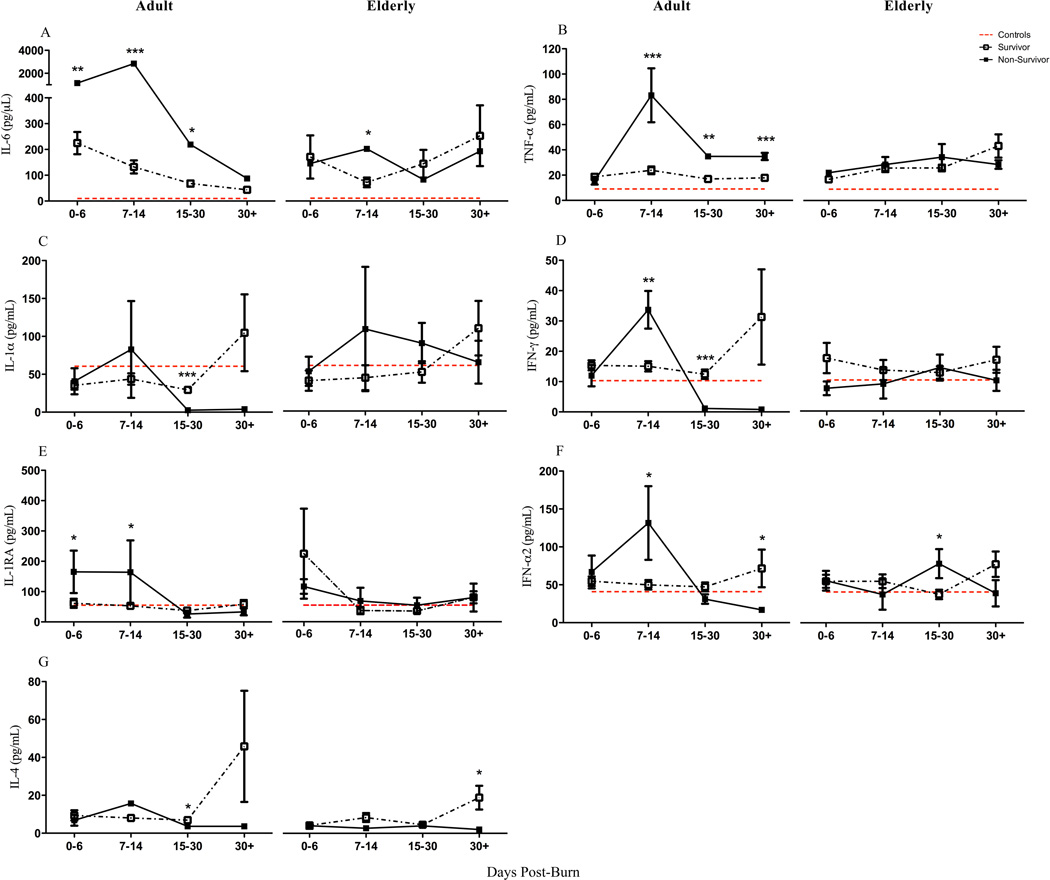
Results: Elderly burn patients had significantly lower burn size but significantly higher Baux scores. Morbidity and mortality was significantly increased in the elderly cohort. Immune biomarkers indicated that elderly are immune compromised and unable to respond with the expected inflammatory response during the early phase after injury. This trajectory changes to a hyperinflammatory pattern during the later phase after burn. These findings are even more pronounced when comparing sepsis versus nonsepsis patients as well as survivors versus nonsurvivors in the elderly.
Conclusions: Elderly burned patients mount a delayed immune and dampened inflammatory response early after burn injury that changes to an augmented response at later time points. Late-onset sepsis and nonsurvivors had an immune exhaustion phenotype, which may represent one of the main mediators responsible for the striking mortality in elderly.
Figures
References
-
- Milan A. Age and sex structure: Canada, provinces and territories, 2010. 2011 Retrieved from http://www.statcan.gc.ca.
-
- Barillo DJ, Goode R. Fire fatality study: demographics of fire victims. Burns. 1996;22:85–88. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
