

Levonorgestrel intrauterine system for endometrial protection in women with breast cancer on adjuvant tamoxifen
- PMID: 26649916
- PMCID: PMC6823262
- DOI: 10.1002/14651858.CD007245.pub3
Levonorgestrel intrauterine system for endometrial protection in women with breast cancer on adjuvant tamoxifen
Update in
-
Levonorgestrel intrauterine system for endometrial protection in women with breast cancer on adjuvant tamoxifen.Cochrane Database Syst Rev. 2020 Dec 21;12(12):CD007245. doi: 10.1002/14651858.CD007245.pub4. Cochrane Database Syst Rev. 2020. PMID: 33348436 Free PMC article.
Abstract
Background: Adjuvant tamoxifen reduces the risk of breast cancer recurrence in women with oestrogen receptor-positive breast cancer. Tamoxifen also increases the risk of postmenopausal bleeding, endometrial polyps, hyperplasia, and endometrial cancer. The levonorgestrel-releasing intrauterine system (LNG-IUS) causes profound endometrial suppression. This systematic review considered the evidence that the LNG-IUS prevents the development of endometrial pathology in women taking tamoxifen as adjuvant endocrine therapy for breast cancer.
Objectives: To determine the effectiveness and safety of levonorgestrel intrauterine system (LNG-IUS) in pre- and postmenopausal women taking adjuvant tamoxifen following breast cancer for the outcomes of endometrial and uterine pathology including abnormal vaginal bleeding or spotting, and secondary breast cancer events.
Search methods: We searched the following databases: Cochrane Menstrual Disorders and Subfertility Group Specialised Register (MDSG), Cochrane Breast Cancer Group Specialised Register (CBCG), Cochrane Central Register of Controlled Trials (CENTRAL), Cochrane Database of Abstracts of Reviews of Effects (DARE), The Cochrane Library, clinicaltrials.gov, The World Health Organisation International Trials Registry, ProQuest Dissertations & Theses, MEDLINE, EMBASE, CINAHL (Cumulative Index to Nursing and Allied Health Literature), PsycINFO, Web of Science, OpenGrey, LILACS, PubMed, and Google. The final search was performed in October 2015.
Selection criteria: Randomised controlled trials of women with breast cancer on adjuvant tamoxifen that compared endometrial surveillance alone (control condition) versus the LNG-IUS with endometrial surveillance (experimental condition) on the incidence of endometrial pathology.
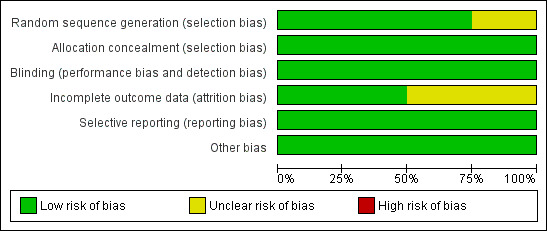
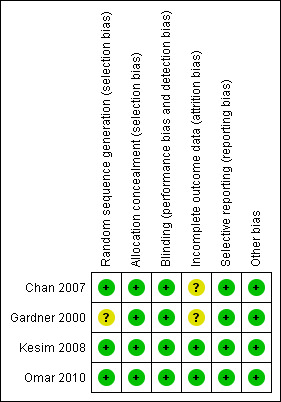
Data collection and analysis: Study selection, risk of bias assessment and data extraction were performed independently by two review authors. The primary outcome measure was endometrial pathology (including polyps, endometrial hyperplasia, or endometrial cancer) diagnosed at hysteroscopy or endometrial biopsy. Secondary outcome measures included fibroids, abnormal vaginal bleeding or spotting, breast cancer recurrence, and breast cancer-related deaths. The overall quality of evidence was rated using GRADE methods.
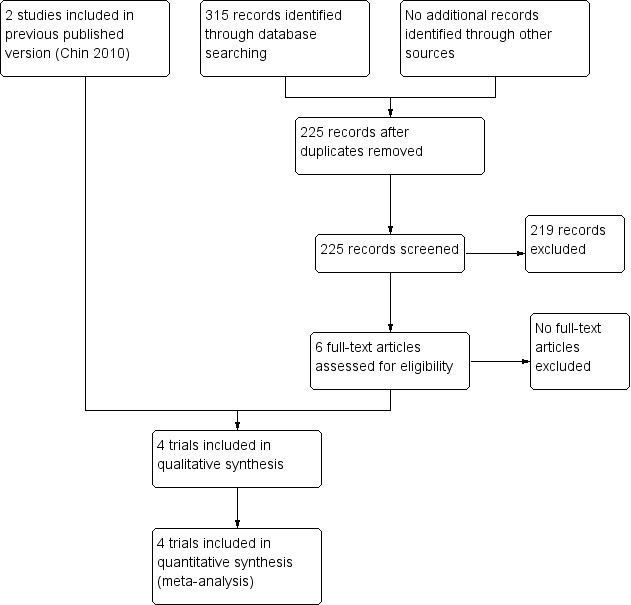
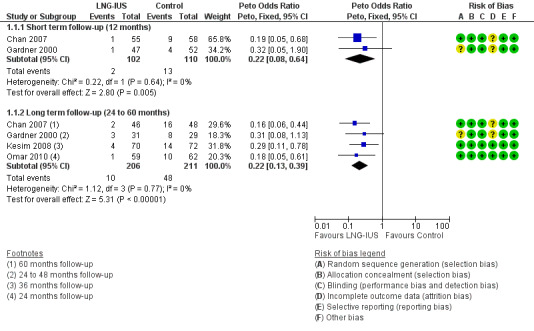
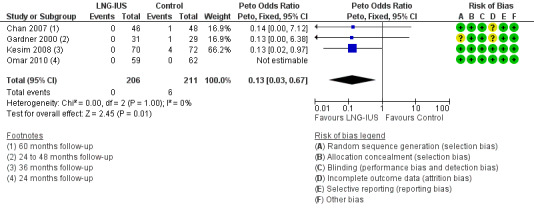
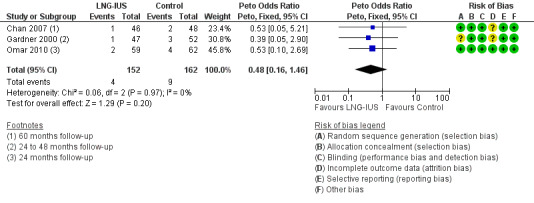
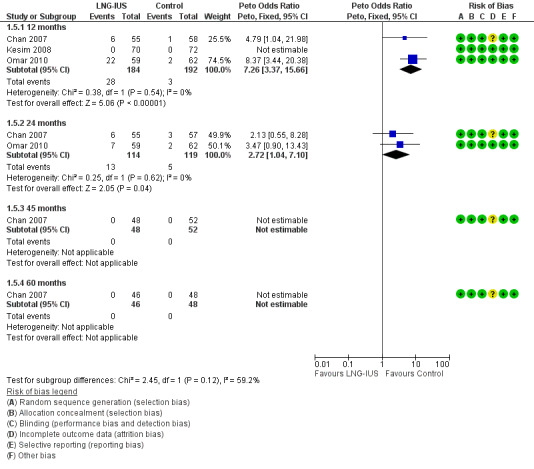
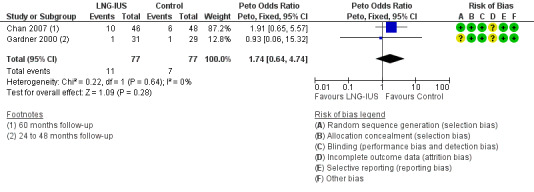
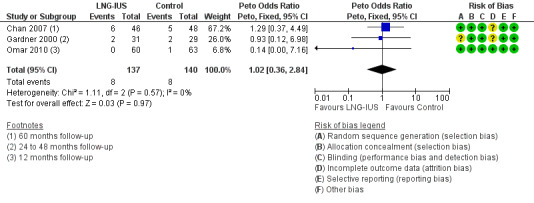
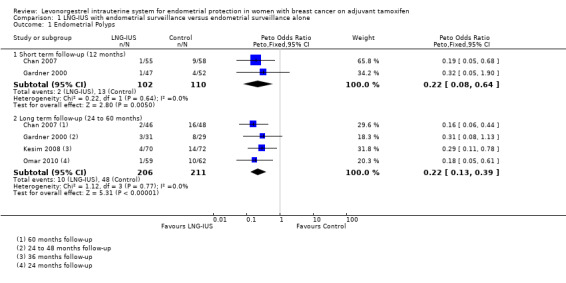
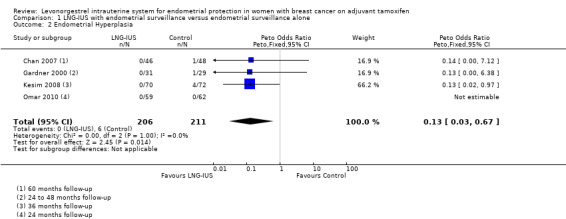
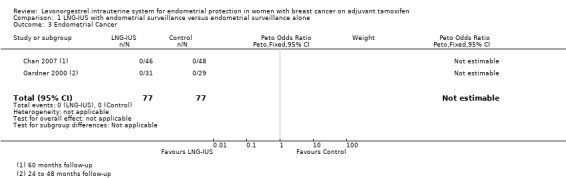
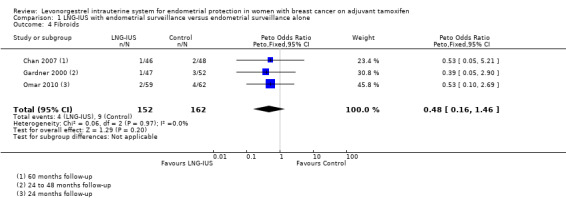
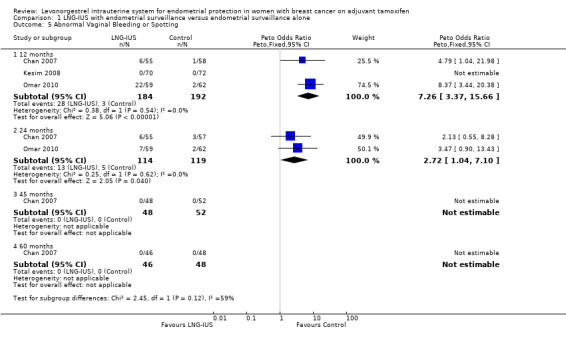
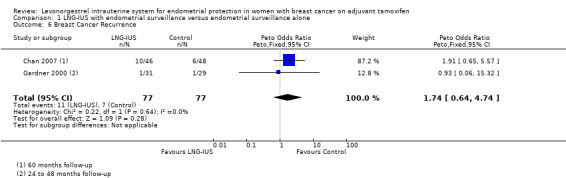
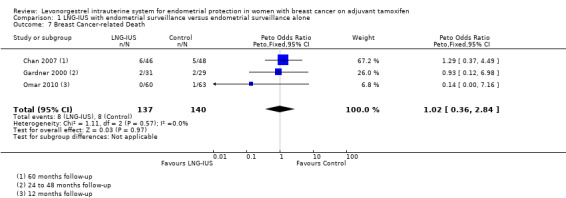
Main results: Four randomised controlled trials involving 543 women were identified and are included in this review. In the included studies, the active treatment arm was the 20 μg/day levonorgestrel-releasing intrauterine system (LNG-IUS) plus endometrial surveillance; the control arm was endometrial surveillance alone. In tamoxifen users, the LNG-IUS led to a reduction in the incidence of endometrial polyps over both a 12-month period (Peto OR 0.22, 95% CI 0.08 to 0.64, 2 studies, n = 212, I² = 0%) and over a long-term follow-up period (24 to 60 months) (Peto OR 0.22, 95% CI 0.13 to 0.39, 4 studies, n = 417, I² = 0%, moderate quality evidence). Also the LNG-IUS led to a reduction in the incidence of endometrial hyperplasia over a long-term follow-up period (24 to 60 months) (Peto OR 0.13, 95% CI 0.03 to 0.67, four studies, n = 417, I² = 0%, moderate quality evidence). However, it should be noted that the number of events of endometrial hyperplasia was low (n = 6). None of the trials were sufficiently powered to detect whether LNG-IUS leads to significant changes in the incidence of endometrial cancer in tamoxifen users. At 12 months of follow-up abnormal vaginal bleeding or spotting was more common in the LNG-IUS treatment group (Peto OR 7.26, 95% CI 3.37 to 15.66, 3 studies, n = 376, I² = 0%, moderate quality evidence). By 24 months of follow-up, abnormal vaginal bleeding or spotting occurred less frequently compared to 12 months of follow-up in the LNG-IUS treatment group but was still more common than the control group (Peto OR 2.72, 95% CI 1.04 to 7.10, 2 studies, n = 233, I² = 0%, moderate quality evidence). By 60 months of follow-up, no cases of abnormal vaginal bleeding or spotting were reported in either group. The numbers of events for the following outcomes were low: fibroids (n = 13), breast cancer recurrence (n = 18), and breast cancer-related deaths (n = 16). There was no evidence of a difference between the LNG-IUS treatment group and controls for these outcomes. The quality of the evidence was judged as moderate, due to limited sample sizes and low event rates for the outcome comparisons.
Authors' conclusions: The LNG-IUS reduces the incidence of benign endometrial polyps and endometrial hyperplasia in women with breast cancer taking tamoxifen. At 12 and 24 months of follow-up, the LNG-IUS increased abnormal vaginal bleeding or spotting among women in the treatment group compared to those in the control. There is no clear evidence from the available randomised controlled trials that the LNG-IUS prevents endometrial cancer in these women. There is no clear evidence from the available randomised controlled trials that the LNG-IUS affects the risk of breast cancer recurrence or breast cancer-related deaths. Larger studies are necessary to assess the effects of the LNG-IUS on the incidence of endometrial cancer, and to determine whether the LNG-IUS might have an impact on the risk of secondary breast cancer events.
Conflict of interest statement
Former review author Professor Justin C Konje is a co‐author for one of the randomised controlled trials included in this review (Gardner 2000).
Figures
Update of
-
Levonorgestrel intrauterine system for endometrial protection in women with breast cancer on adjuvant tamoxifen.Cochrane Database Syst Rev. 2009 Oct 7;(4):CD007245. doi: 10.1002/14651858.CD007245.pub2. Cochrane Database Syst Rev. 2009. Update in: Cochrane Database Syst Rev. 2015 Dec 09;(12):CD007245. doi: 10.1002/14651858.CD007245.pub3. PMID: 19821400 Updated.
References
References to studies included in this review
Chan 2007 {published data only}
-
- Chan SSC, Tam WH, Yeo W, Yu MMY, Ng DPS, Wong AWY, et al. A randomised controlled trial of prophylactic levonorgestrel intrauterine system in tamoxifen treated women. BJOG 2007;114(12):1510–5. - PubMed
-
- Wong AWY, Chan SSC, Yeo W, Yu MY, Tam WH. Prophylactic use of levonorgestrel‐releasing intrauterine system in women with breast cancer treated with tamoxifen: a randomized controlled trial. Obstetrics and Gynecology 2013;121(5):943‐50. - PubMed
Gardner 2000 {published data only}
-
- Gardner FJE, Konje JC, Abrams KR, Brown LJR, Khanna S, Al‐Azzawi F, et al. Endometrial protection from tamoxifen‐stimulated changes by a levonorgestrel‐releasing intrauterine system: a randomised controlled trial. Lancet 2000;356(9243):1711‐7. - PubMed
-
- Gardner FJE, Konje JC, Bell SC, Abrams KR, Brown LJ, Taylor DJ, Habiba M. Prevention of tamoxifen induced endometrial polyps using levonorgestrel releasing intrauterine system: Long‐term follow‐up of a randomised control trial. Gynecologic Oncology 2009;114(3):452‐6. - PubMed
Kesim 2008 {published data only}
-
- Kesim MD, Aydin Y, Atis A, Mandiraci G. Long‐term effects of the levonorgestrel‐releasing intrauterine system on serum lipids and the endometrium in breast cancer patients taking tamoxifen. Climacteric 2008;11(3):252‐7. - PubMed
Omar 2010 {published data only}
-
- Omar H, Elkhayat W, Aboulkasem M. The use of levonorgestrel‐releasing intrauterine system in prevention of endometrial pathology in women with breast cancer treated with tamoxifen. The International Journal of Medicine 2010;3(1):327‐330.
Additional references
ACOG 2006
-
- ACOG Committee Opinion No 336. Tamoxifen and uterine cancer. Obstetrics and Gynecology 2006;107(6):1475‐8. - PubMed
Coates 2007
-
- Coates AS, Keshaviah A, et al. Five years of letrozole compared with tamoxifen as initial adjuvant therapy for postmenopausal women with endocrine‐responsive early breast cancer: update of study BIG 1‐98. Journal of Clinical Oncology 2007;10;25(5):486‐92. - PubMed
Cohen 2004
-
- Cohen I. Endometrial pathologies associated with postmenopausal tamoxifen treatment. Gynecologic Oncology 2004;94(2):256‐66. - PubMed
Davies 2013
-
- Davies C, Pan H, Godwin J, Gray R, Arriagada R, et al for the Adjuvant Tamoxifen: Longer Against Shorter (ATLAS) Collaborative Group. Long‐term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor‐positive breast cancer: ATLAS, a randomised trial. Lancet 2013;381(9869):805‐816. - PMC - PubMed
EBCTCG 2005
-
- Early Breast Cancer Trialists Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15‐year survival: an overview of the randomised trials. Lancet 2005;365(9472):1687‐717. - PubMed
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Kedar 1994
-
- Kedar RP, Bourne TH, Powles TJ, Collins WP, Ashley SE, Cosgrove DO, et al. Effects of tamoxifen on uterus and ovaries of postmenopausal women in a randomized breast cancer prevention trial. Lancet 1994;343:1318‐21. - PubMed
Lyytinen 2009
-
- Lyytinen HK, Dyba T, Ylikorkala O, Pukkala EI. A cases control study on hormone therapy as a risk factor for breast cancer in Finland. International Journal of Cancer July 2009;126(2):483‐9. - PubMed
Scommegna 1970
-
- Scommegna A, Pandya GN, Christ M, Lee AW, Cohen MR. Intrauterine administration of progesterone by a slow releasing device. Fertility and Sterility 1970;21(3):201‐10. - PubMed
Trinh 2008
-
- Trinh XB, Tjalma WA, Makar AP, Buytaert G, Weyler J, Dam Pa. Use of the levonorgestrel‐releasing intrauterine system in breast cancer patients. Fertility and Sterility 2008;90(1):17‐22. - PubMed
Van Leeuwen 1994
-
- Leeuwen FE, Benraadt J, Coesbergh JW, Kiemeney LA, Gimbrere CH, Otter R. Risk of endometrial cancer after tamoxifen treatment of breast cancer. Lancet 1994;343:1318‐21. - PubMed
www.cancer.org
-
- American Cancer Society. www.cancer.org. www.cancer.org 2008.
Xiao 1990
-
- Xiao BL, Zhou LY, Zhang XL, Jia MC, Luukkainen T, Allonen H. Pharmacokinetic and pharmacodynamic studies of levonorgestrel‐releasing intrauterine device. Contraception 1990;41(4):353‐62. - PubMed