

The Rotterdam Scan Study: design update 2016 and main findings
- PMID: 26650042
- PMCID: PMC4690838
- DOI: 10.1007/s10654-015-0105-7
The Rotterdam Scan Study: design update 2016 and main findings
Abstract
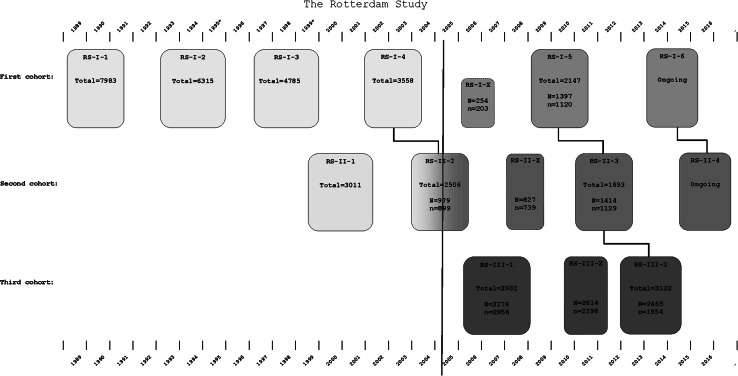
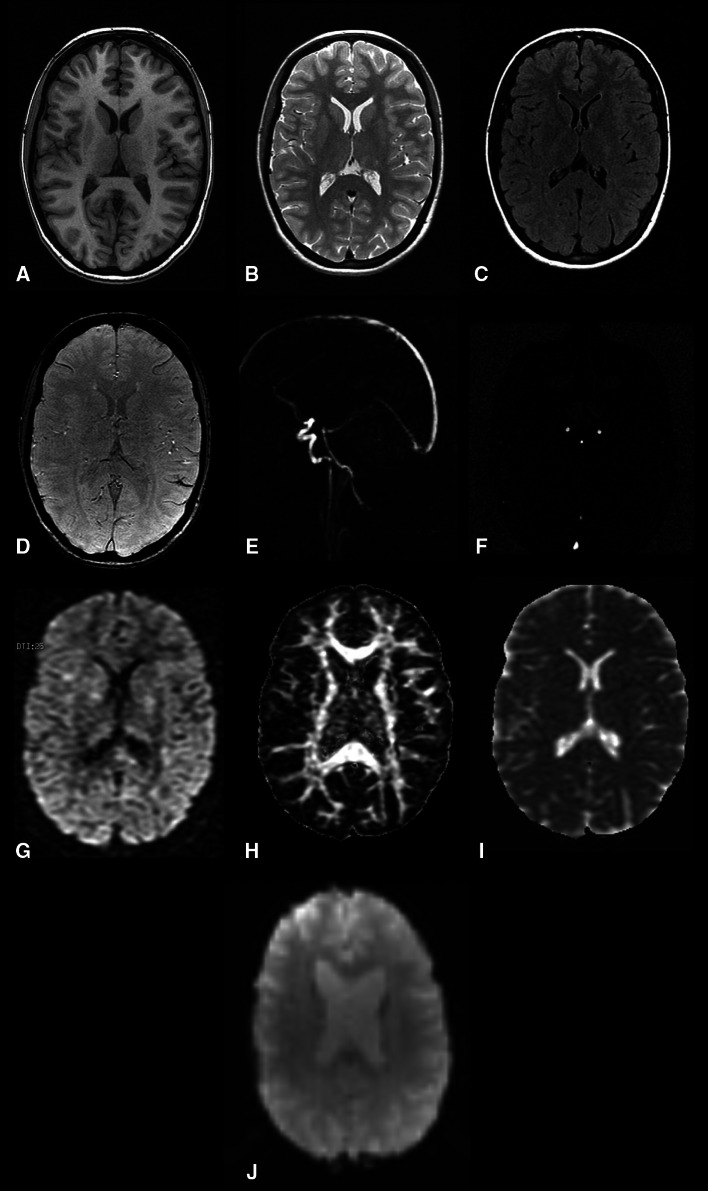
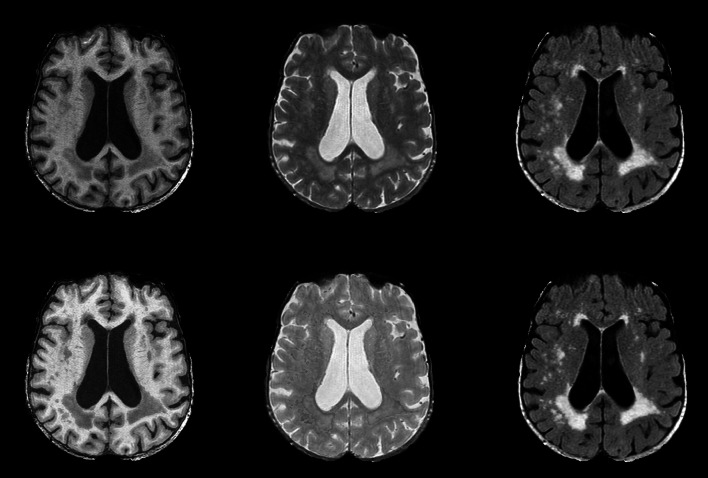
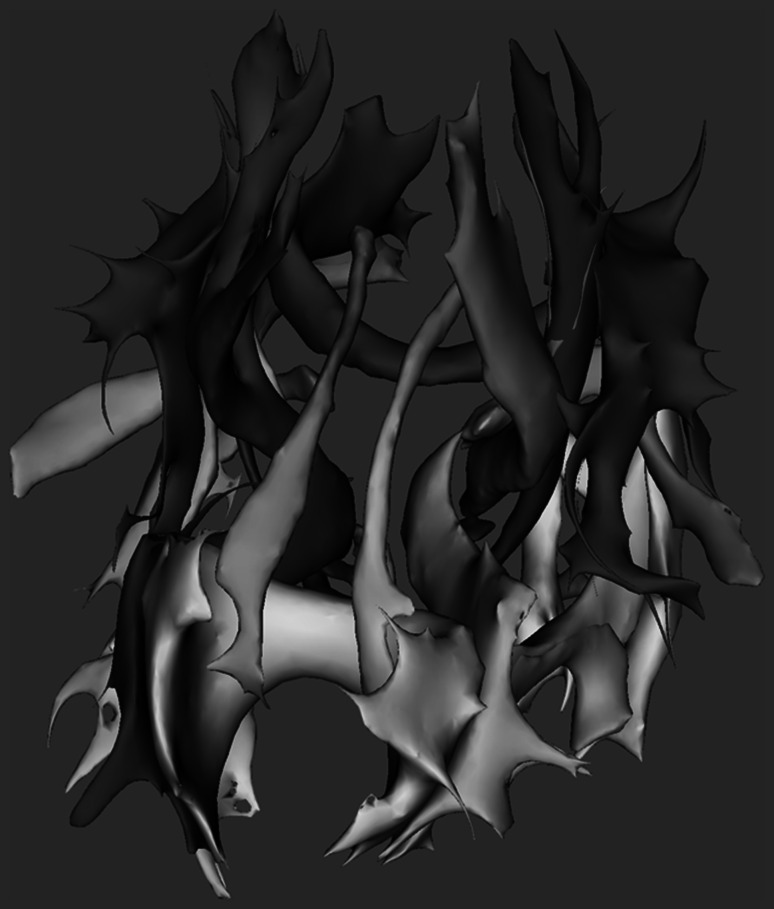
Imaging plays an essential role in research on neurological diseases in the elderly. The Rotterdam Scan Study was initiated as part of the ongoing Rotterdam Study with the aim to elucidate the causes of neurological disease by performing imaging of the brain in a prospective population-based setting. Initially, in 1995 and 1999, random subsamples of participants from the Rotterdam Study underwent neuroimaging, whereas from 2005 onwards MRI has been implemented into the core protocol of the Rotterdam Study. In this paper, we discuss the background and rationale of the Rotterdam Scan Study. Moreover, we describe the imaging protocol, image post-processing techniques, and the main findings to date. Finally, we provide recommendations for future research, which will also be topics of investigation in the Rotterdam Scan Study.
Keywords: Alzheimer’s disease; Cerebral blood flow; Cohort study; Dementia; Diffusion tensor imaging; Epidemiology; Genetics; Infarcts; Microbleeds; Neuroimaging; Population-based; Risk factors; Stroke; White matter lesions.
Figures
References
-
- Hachinski V. Stroke and Alzheimer disease: fellow travelers or partners in crime? Arch Neurol. 2011;68(6):797–798. - PubMed
-
- Seshadri S, Wolf PA, Beiser A, Au R, McNulty K, White R, et al. Lifetime risk of dementia and Alzheimer’s disease. The impact of mortality on risk estimates in the Framingham Study. Neurology. 1997;49(6):1498–1504. - PubMed
-
- Seshadri S, Wolf PA. Lifetime risk of stroke and dementia: current concepts, and estimates from the Framingham Study. Lancet Neurol. 2007;6(12):1106–1114. - PubMed
-
- Thies W, Bleiler L. 2011 Alzheimer’s disease facts and figures. Alzheimers Dement. 2011;7(2):208–244. - PubMed
-
- Meyer JS, Kawamura J, Terayama Y. White matter lesions in the elderly. J Neurol Sci. 1992;110(1–2):1–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
